 As posted on BIJC before, Asad et al. had performed a systematic review on the usage of ketamine as a continuous infusion (>24h) in intensive care patients. The same authors have now published a narrative review providing a more depth discussion about the pharmacological and pharmacokinetic properties of ketamine. Also they present recommendations for dosing and monitoring in an ICU setting. The Goodies of KetCurrent evidence shows that Ketamine... - Has no adverse effects on the gastrointestinal tract (bleeding) and does not cause acute kidney injury (compared to nonsteroidal anti-inflammatory drungs, NSAID's) - Does not negatively influence bowel motility (in contrast to opioids) - Preserves laryngeal protective reflexes - Lowers airway resistance - Increases lung compliance - Is less likely to cause respiratory depression - Is sympathomimetic, facilitates adrenergic transmission and inhibits synaptic catecholamine reuptake, therefore increasing heart rate and blood pressure The Concerns of KetKetamine... - Might increase pulmonary airway pressure and therefore aggravate pulmonary hypertension - Might cause well known psychotomimetic effects which are of concern in the critically ill patient as this might predispose to delirium - Interacts with benzodiazepines via the P450 pathway which could result in drug accumulation and prolonged recovery Concerns Proven Wrong- Ketamine need not to be avoided in patients at risk for seizures, particularly when used for analgosedation for short periods in the ICU setting - Current evidence shows no increased intracranial pressure or associated adverse neurologic outcomes associated with ketamine administration in critically ill patients Take HomeThe use of ketamine for analgosedation in the ICU continues to lack high-level evidence.However, it is effectively used around the globe and remains an attractive alternative agent for appropriately selected patients. Taking current knowledge and evidence into account this is especially true for patients with severe pain unresponsive to conventional therapies.
Taking precautions and contraindications into account ketamine is considerably safe and even avoids potentially adverse side effects of other agents used. Erstad BL, J Crit Care, Oct 2016, Vol 35, p 145-149 The Problem An endogenous Cushing's syndrome, mostly caused by an adenoma of the pituitary gland, is associated with significant morbidity and mortality when left untreated. The condition is closely associated to life-threatening infections, diabetes mellitus, hypertension and increased risk associated with surgery. For Cushing's disease the first line therapy is surgical removal of the pituitary tumor. Sometimes though urgent medical therapy is needed first. It has been shown, that surgical risk may be significantly reduced if cortisol concentrations are normalised preoperatively. Conditions requiring urgent cortisol-lowering measures are severe biochemical disturbances (e.g. hypokalaemia), immunosuppression or mental instability. Medical Treatment OptionsKetokonazole (yes, the antifungal agent) and metyrapone are used to suppress adrenal steroidogenesis at enzymatic sites. Both agents carry the risk of postential side effects. Mifepristone, a glucocorticoid receptor antagonist, and pasireotide, a new targeted pituitary therapy, are alternative agents. However, they also have their limits and side effects. EtomidateNow that's where etomidate joins the game. Interestingly, etomidate and ketokonazole are chemically closely related... they are both members of the imidazole family. Etomidate is used as an anaesthetic agent since 1972 and became popular for hemodynamic stability and the lack if histamine release. In 1983 a Lancet article noted an increased mortality when etomidate was used in critically unwell patients. In 1984 an article in Anaesthesia first showed a link to low serum cortisol levels caused by etomidate. Until now the discussion continues, whether a single induction dose actually negatively influences patient outcome. A meta-analysis in 2010 was unable confirm this apprehension and the debate continues. Fact isEtomidate suppresses the production of cortisol by inhibiting the mitochondrial cytochrome p450-dependent adrenal enzyme 11-beta-hydroxylase and therefore lower serum cortisol levels within 12 hours. In higher doses it also blocks side chain cleavage enzymes and also aldosterone synthase. It might even have anti-proliferative effects on adrenal cortical cells. On this basis the idea arose, that etomidate might be a useful therapy for severe hypercortisolaemia. Continuous Etomidate - What's the EvidenceA review article by Preda et al. in 2012 identified 18 publications about the primary therapeutic usage of etomidate in Cushing's syndrome, most of which were case reports. Review of current literature reveals that etomidate indeed suppresses hypercortisolaemia safely and efficiently in patients requiring parenteral therapy. Moreover, etomidate shows a dose-dependent suppression and allows adjustment of the medication to target cortisol levels. At recommended dosages etomidate is considered safe with almost no serious side effects. The authors conclude, that etomidate is a useful therapeutic option in a hospital setting when oral therapy is not tolerated or inappropriate. Take home- Continuous etomidate (in non-hypnotic doses) reduces cortisol concentrations in a dose-dependent manner in both hyper- and eucortisolaemic subjects - The application of continuous etomidate in Cushing's disease is safe and efficient - After termination of infusion adrenocortical suppression persists for about 3 hours - The suspicion, that a single dose of etomidate for rapid sequence inductions might negatively influence patient outcome in the critically ill remains a matter of debate J Clin Endocrinol Metab. 1990 May;70(5):1426-30. Preda et al. European Journal of Endocrinology (2012) 167 137-143 OPEN ACCESS Soh et al. Letter to the Editor, European Journal of Endocrinology (2012) 167 727–728 Ge et al. Critical Care201317:R20 OPEN ACCESS 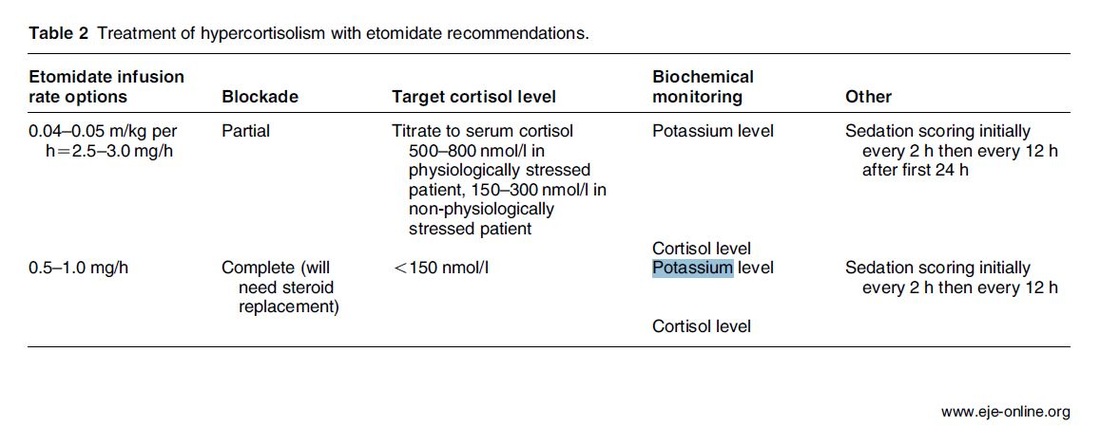  Fluids are one of the cornerstones in the treatment of patients with shock. But with any drug applied, also fluids can harm if given inappropriately! While inadequate fluid resuscitation might result in tissue hypoperfusion and worsening of end-organ function, to much fluid might lead to problems like pulmonary oedema and finally increased mortality. Many measures are used in clinical practice, but most of them lack specificity and are not very representative as a sole marker. One of the better methods to evaluate fluid requirements is the use of dynamic measures that estimate the change in cardiac output (CO) in response to a fluid bolus. In this regard the use of point-of-care ultrasound (POCUS) has become increasingly attractive in order to use basic critical care ultrasound to asses the need of fluids in a specific clinical setting. Lee at al. have now looked at the sonographic assessment of the inferior vena cava and lung ultrasound in order to quite fluid therapy in intensive care. By taking into account current evidence they have produced an algorithm using these measures to help guiding fluid therapy. As with any measurement in critically ill patients the pathophysiologic cause of shock must be taken into account. The algorithm presented here seems to work best in patients in hypovolemic shock. To fully understand the following algorithm and its limitations we recommend to read the open access article (see link below). In conclusion: The algorithm provided is a helpful tool to help assess the need of fluids in a simple and quick manner. Lee C et al. J of Crit Care 31 (2016) 96-100 OPEN ACCESS 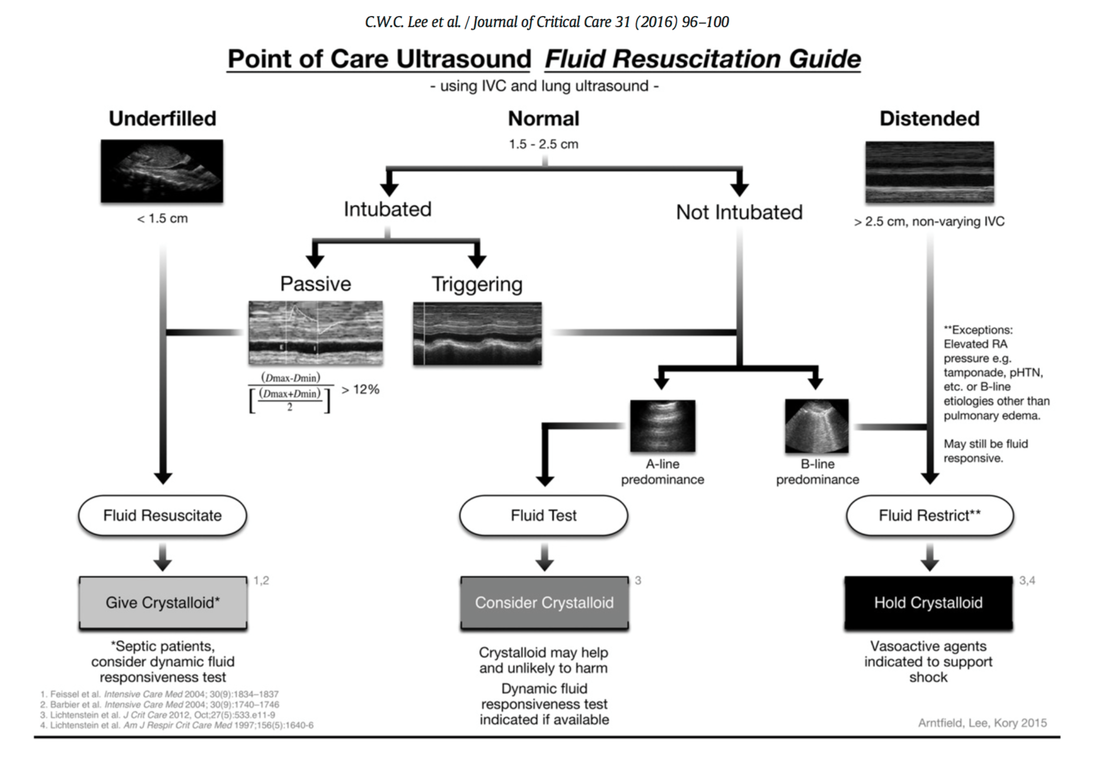  Sepsis certainly keeps us going... either when treating patients on ICU or when it comes to the discussion on what actually sepsis is and how to define it. So far the SIRS (Systemic Inflammatory Response Syndrome) criteria have provided some degree of handle to cope with this syndrome but of course we weren't all quite happy with this. In fact every person with any sort of infectious disease will respond with 2 or more SIRS criteria... but doesn't necessarily have to be septic. As a matter of fact a SIRS is nothing else but a physiologic response to any sort of inflammation. The New Approach to Sepsis - The SOFA The new international consensus definitions for sepsis and septic shock try to focus on the fact that sepsis itself defines a life-threatening organ dysfunction caused by a dysregulated host response to infection. By saying this the aim is to provide a definition that allows early detection of septic patients and allow prompt and appropriate response. As even a modest degree of organ dysfunction is associated with an increased in-hospital mortality the SOFA score (Sequential or 'Sepsis-related' Organ Failure Assessment) was found to be the best scoring system for this purpose. It's well known, simple to use and has a well-validated relationship to mortality risk. Sepsis (related organ dysfunction) is now defined by a SOFA score increase of 2 points or more 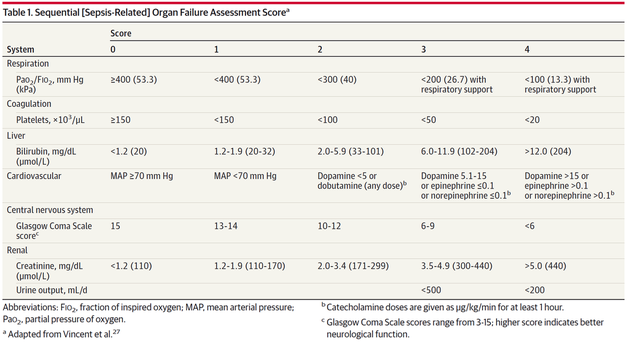 The Quick Approach to Sepsis - The BAT In the out-of-hospital setting, on the general wards or in the emergency department the task force recommends an altered bed side clinical score called the quickSOFA - or alternatively 'the BAT' score: 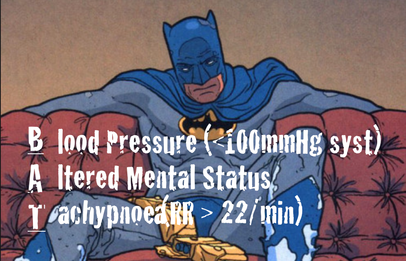 The New Approach to Septic Shock -Vasopressors and Lactate Septic shock is now defined as a subset of sepsis in which underlying circulatory, cellular, and metabolic abnormalities are associated with a greater risk of death than sepsis alone. Keeping a long story short: Septic Shock is now: - The need for vasopressors to maintain a mean arterial pressure of at least 65mmHg AND - a serum lactate level of more than 2mmol/L... after adequate fluid resuscitation 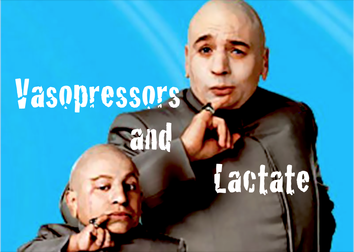 The Bottom Line: The way it looks like we are left with Sepsis and Septic Shock Severe Sepsis has vanished and the question remains, whether these new definitions will actually benefit the ones that need it most... our septic patients! Singer M et al. JAMA. 2016;315(8):801-810. Seymour CW et al. JAMA. 2016;315(8):762-774. Shankar-Hari M et al. JAMA. 2016;315(8):775-787.  One of the most controversial manoeuvres in anaesthesia and critical care has got some new support since the Difficult Airway Society has published their new guidelines in which they basically continue to support the use of cricoid pressure (CP) for rapid sequence induction. The authors of the Obstetric Anaesthetists' Association and Difficult Airway Society Guidelines for the Management of Difficult and Failed Tracheal Intubation also continue to recommend routine CP, which is considered level 3b evidence.
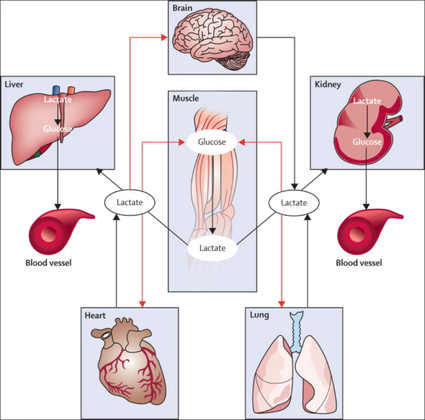
Surprised on how obstinately CP persists in current guidelines I think that following statement by Priebe HJ is an important reading. It summarises nicely why there is such a disagreement with these recommendations. He states that - not a single controlled clinical study provided convincing evidence that the use of cricoid pressure was associated with a reduced risk of pulmon ary aspiration. At the same time, there is good evidence that nearly all aspects of airway management are adversely affected by cricoid pressure - if cricoid pressure were considered a new airway device, it would not be considered for further evaluation because Level 3B evidence for its efficacy does not exist - when using cricoid pressure, we may well be endangering more lives by interfer ing with optimal airway management than we are saving lives by preventing pulmonary aspiration Priebe HJ, Anaesthesia 2016, 71, 343–351 Want to get more information on the controversy of cricoid pressure? Read here: Cricoid Pressure for RSI in the ICU: Time to Let GO? Time to let go? Remarkable article on RSI and Cricoid Pressure Difficult Airway Society DAS: New Guidelines OUT! Cricoid Pressure still IN?  The discussion on the so-called lactic acidosis and its causes have become increasingly attractive over the last couple of years as several biochemical explanations are challenged. A significant confusion persists on the various relationships between lactate, lactic acid and metabolic acidosis. Most clinicians continue to refer to the traditional understanding of impaired tissue oxygenation causing increased lactate production, impaired lactate clearance and therefore resultant metabolic acidosis. Just recently we had a discussion on our ward round on this topic when a team member presented the most recent article of UpToDate online on the causes of lactic acidosis. The authors state that 'Lactic acidosis is the most common cause of metabolic acidosis in hospitalised patients' and that 'Lactic acidosis occurs when lactate production exceeds lactate clearance. The increase in lactate production is usually caused by impaired tissue oxygenation...'... finally suggesting that lactate is no good! These statements support the classical understanding that: - Hyperlactatemia is caused by tissue hypoxemia, and - This in turn then leads to a metabolic acidosis called lactic acidosis This biochemical understanding has persisted for decades, but there are some good reasons to vigorously challenge this traditional aspect on the 'bad' lactate. Lactate turns out to be by far more complex in its characteristics and functions, so I decided to try and make a short but comprehensive overview of this molecule. What is lactate? Lactate is a small organic molecule with the chemical formula CH3CH(OH)CO2H and structurally looks like on the image to the left. It is produced in the cytoplasm of human cells mainly by anaerobic glycolysis by the conversion of pyruvate to lactate by LDH. This chemical reaction results typically in a blood lactate to pyruvate ratio of about 10:1. And while lactate is produced, NAD+ also is incurred, and this actually can accept protons itself, so does not result in acidosis itself. Lactate arises from the production of energy by consuming glycogen and glucose. 
|
|||||










| Click here to read |

As knowledge is growing the ATS, ERS, JRS and ALAT (... thoracic and respiratory societies) made the effort to look into the latest evidence by performing systematic reviews and where appropriate meta-analyses. The aim was to update the guidelines published in 2011. These guidelines are also dedicated to Mr. William Cunningham who actively participated in the development of these guidelines, suffered from idiopathic pulmonary fibrosis for many years and who was directly confronted with the issues related with this condition.
The main conclusions can be briefly summarised as follows:
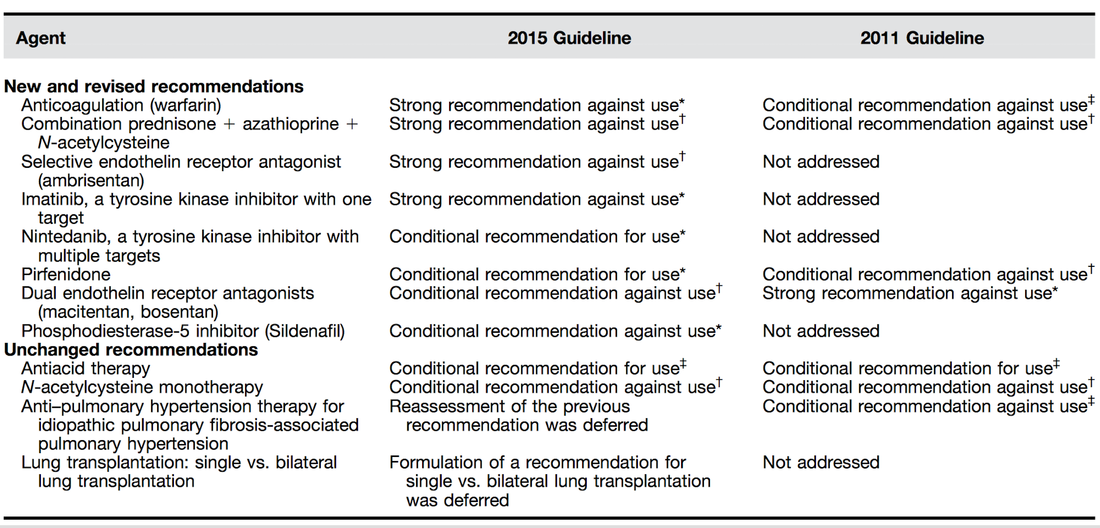
An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline: Treatment of Idiopathic Pulmonary Fibrosis. An Update of the 2011 Clinical Practice Guideline, American Journal of Respiratory and Critical Care Medicine, Vol. 192, No. 2 (2015), pp. e3-e19.
OPEN ACCESS: Executive Summary 2015
An Official ATS/ERS/JRS/ALAT Statement: Idiopathic Pulmonary Fibrosis: Evidence-based Guidelines for Diagnosis and Management, Am J Respir Crit Care Med Vol 183. pp 788–824, 2011 OPEN ACCESS
For further information on acute exacerbations of IPF we recommend this Review Article:
| Acute Exacerbations in Patients with IPF,Kim Respiratory Research 2013, 14:86 |
Search
Translate
Select your language above. Beware: Google Translate is often imprecise and might result in incorrect phrases!

Categories
All
Airway
Cardiovascular
Controversies
Endocrinology
Fluids
For A Smile ; )
Guidelines
Infections
Meducation
Neurology
Nutrition
Pharmacology
Procedures
Radiology
Renal
Respiratory
Resuscitation
SARS CoV 2
SARS-CoV-2
Sedation
Sepsis
Transfusion
Archives
January 2021
September 2020
March 2020
February 2020
January 2020
December 2019
November 2019
July 2019
May 2019
March 2019
February 2019
January 2019
December 2018
January 2018
October 2017
August 2017
June 2017
March 2017
February 2017
January 2017
October 2016
July 2016
June 2016
April 2016
February 2016
December 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
Author
Timothy Aebi
 RSS Feed
RSS Feed


