 As mentioned in one of our earlier entries two important trials (Hermanns et al. The Lancet and Caesar et al. NEJM) have indicated that early parenteral nutrition (PN) might actually be harmful and a late PN strategy should be the standard of care.
Despite this the debate has continued and remains highly controversial. This is nicely reflected in recent guidelines regarding the timing of supplemental PN. While the European Society for Clinical Nutrition and Metabolism (ESPEN) recommends PN within 24-48h in patients who are expected to be intolerant to enteral nutrition (EN), the American Society for Parenteral and Enteral Nutrition (ASPEN) recommends postponing the initiation of PN until day 8 after ICU admission. In order to clarify things a little Bost et al. have now published a systematic review on the timing of parenteral nutrition in critical care (Open access). From 3520 initially screened articles only four randomised controlled trials and two prospective observational studies remained after critical appraisal. "In conclusion it seems to be reasonable to assume that in critically ill patients, when full enteral support is contraindicated or fails to reach caloric targets, there are no clinically relevant benefits of early PN compared to late PN with respect to morbidity or mortality end points. Considering that infectious morbidity and resolution of organ failure may be negatively affected through mechanisms not yet clearly understood and acquisition costs of parenteral nutrition are higher, the early administration of parenteral nutrition cannot be recommended." The Review in one short sentence: Early PN has no advantage over late PN, but might be actually harmful. Bost et al. Annals of Intensive Care 2014, 4:31 Read more: ESPEN Guidelines on parenteral nutrition, 2009 A.S.P.E.N. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient BIJC.org on: Starting early PN weakens the critically ill  Several studies in the past have looked into the topic of red blood cell (RBC) transfusions in the ICU and each one of them supports a rather restrictive approach in the ICU. Still though various guidelines around the world vary due to the lack of evidence (see below).
This october the New England Journal of Medicine (unnoticeably and slowly transforming into a critical care journal ;) published a large multi-centered, partially blinded trial that randomised septic patients in intensive care units to receive RBC at a threshold of 70g/L or 90g/L. The primary outcome was mortality after 90 days. A total of 998 patients finally underwent randomisation and as a result there was no significant difference in mortality after 90 days. Also there were no statistically significant differences in all secondary endpoints like use of life supporting measures, ischemic events, and severe adverse reactions. This trial adds up to a list of studies showing that a liberal transfusion strategy is not beneficial for patients in critical care. This seems to be especially true for patients with sepsis. And not to forget: a considerable amount of packed RBC can be saved this way. A higher transfusion threshold of 90g/L in patients with sepsis is non-superior to a lower threshold of 70g/L. Get an insight into this topic yourself, here's the 'must read's about transfusions: The TRICC trial The CRIT study Sherwood M et al. JAMA. 2014 Feb 26;Vol 311, No.8 The FOCUS trial A short educational overview can be found here: http://lifeinthefastlane.com/education/ccc/blood-transfusion-in-icu/ Clinical Practice Guidelines from the AABB 2012: Ann Inten Med. 2012;157:49-58 Clinical Practice Guidelines 2009: Red blood cell transfusion in adult trauma and critical care, Crit Care Med 2009  The Lancet has now published the multi-centre study (PROVHILO) which has looked at the role of positive end-expiratory pressure (PEEP) for mechanical ventilation during general anaesthesia. For that reason the PROVE network investigators have included almost 900 patients in a randomised controlled trial who were planned for open abdominal surgery. All patients were ventilated with a tidal volume (Vt) of 8ml/kg. One group received a PEEP of 12 cmH2O and recruitement maneuvres while the other group got alomst no PEEP (<2 cmH2O) and no recruitement maneuvres. Primary endpoint were pulmonary compications on day 5 postoperatively. They found no difference in pulmonary complications but significantly more introperative hypotension and use of vasoactive agents in the higher PEEP group.
So the investigators conclude that a higher level of PEEP and recruitment maneuvres do not protect against postoperative pulmonary complications. They actually advise to use low tidal volumes and very low PEEP for intraoperative ventilation. The multicenter study is well designed and performed but some questions remain: Why is PEEP never adjusted to weight? One striking feature is that we all use tidal volumes according to the patients body weight, but interestingly nobody seems to use this adjustement for weight when it comes to PEEP. Using a PEEP of 12 in a small and slim 50kg patient has a different impact compared to a massively obese patient. Is 12 cmH2O too high? A PEEP of 12 can be considered generally high and is not used by most anaesthetists in their daily practice anyway. There was no third arm using intermediate levels of PEEP to answer the question on how these patient might have performed. Why did other trial find differing conclusions? The aspect of different levels of PEEP is interesting as previous studies actually were able to show improved outcome with 'protective' mechanical ventilation. The IMPROVE trial in the NEJM from Augut 2013 compared patients for abdominal surgery ventilated with Vt of 10-12ml/kg and 0 cmH2O of PEEP to patients ventilated with Vt of 6-8ml/kg and 6-10 cmH2O of PEEP. In this multicenter, double blind trial with 400 patients improved outcome and reduced health care utilazation were found in the group 'protectively' ventilated. In june 2013 Anaesthesiology published a prospective randomized small trial with 56 patients undergoing open abdominal surgery for more than 2 hours. This time they compared Vt of 9ml/kg and O PEEP to Vt of 7ml/kg and 10 PEEP. This time 'protective' ventilation with PEEP improved respiratory function but did not affect length of hospital stay. Taking these fact into account I think we remain with following conclusions: - The PROVHILO trial is not reason enough to abandon PEEP for anaesthetic ventilation in theatre - Instead we might have to consider adjusting PEEP to the patients clinical condition (e.g. weight) - There is no evidence currently to recommend routine recruitment maneuvers in theatre The Prove Network Investigators, The Lancet, Early Online Publication, 1 June 2014  Ketamine - a drug with various actions and just as many opinions on it. One concern often mentioned is that ketamine might cause a raise in intracranial pressure (ICP) and therefore is often avoided in this group of patients. In May's Journal of Anaesthesia Wang et al. looked at the existing evidence on this topic. They ended up with 5 trials meeting their inclusion criteria on administration of ketamine and the ICP levels within the first 24h as a primary outcome.
To make it short: Ketamine does not increase ICP in comparison to opioids. They conclude that ketamine should not be discouraged on the basis of ICP-related concerns. Wang et al. J Anaesth. 2014 May 24  In the most recent edition of 'Continuing Education in Anaesthesia, Critical Care and Pain' there is a very good overview article on rapid sequence induction (RSI) and its place in modern anaesthesia. Wallace and McGuire also critically look at cricoid pressure (CP) as a part of classical RSI. In their publication they state that "there have been no prospective randomized clinical studies performed to prove the clinical hypothesis and the level of evidence to support the use of cricoid pressure is poor (Level 5)". Level 5 corresponds to 'Expert Opinion' (see table below). They also mention that aspiration has occured despite CP, that CP is often poorly performed, that it may hinder bag-valve mask ventilation as well as LMA insertion and that is may worsen laryngoscopy. It's mentioned that "Critically, it has also been shown to potentially obstruct the upper airway and reduce time to desaturation". 'This is nothing new' you might say. Why am I mentioning this? Well, the remarkable thing about this article is the fact that it was published in a Journal that is a joint venture of the British Journal of Anaesthesia BJA and The Royal College of Anaesthetists in collaboration with the Intensive Care Society and Pain Society. Considering the fact that The NAP4 guidelines continue to support its use as part of an RSI and as such, it is still considered a standard of care in the UK and therefore also Ireland, this publication might indicate some change in mind... or not? The authors summarize: Application of cricoid pressure is advisable — unless it obscures the view at laryngoscopy or interferes with manual ventilation or supraglottic airway device placement. I personally still would want to know what exactly makes a 'Level 5' medical intervention 'advisable' especially in regards of all the possible problems and complications associated with it. Wallace et al., Continuing Education in Anaesthesia, Critical Care & Pain, Volume 14(3), June 2014, p 130–135 Read our previous BIJC post: Cricoid Pressure for RSI in the ICU: Time to Let Go? (Updated) 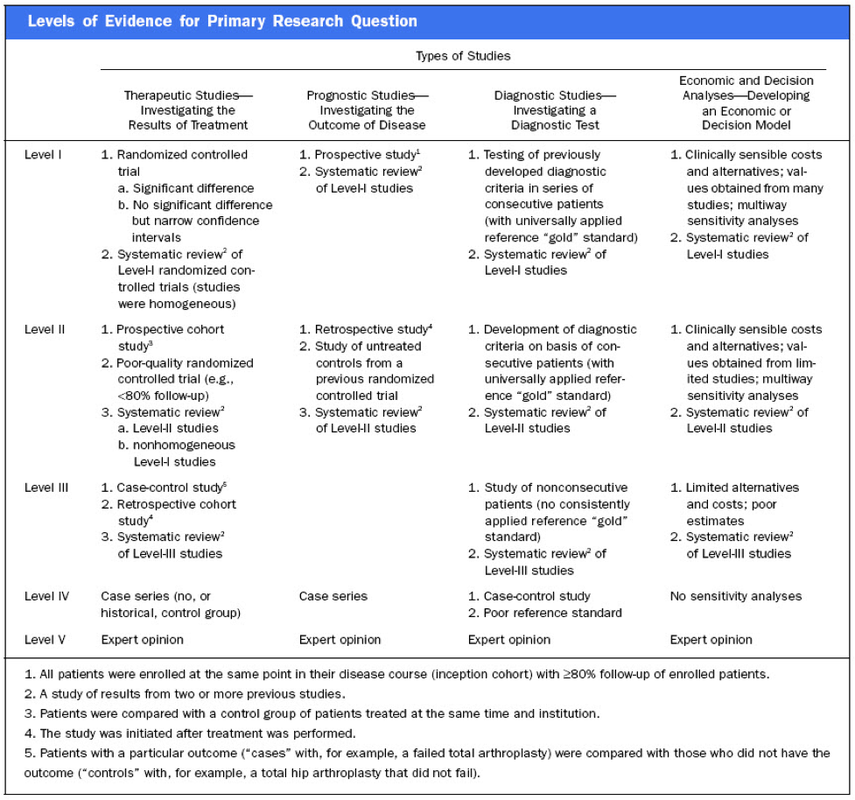  Antibiotic-associated diarrhoea and antibiotic induced Clostridium difficile diarrhoea are a constant problem in the ICU, especially in the elderly patient. There is still some debate going on about prescribing lactobacilli or bifidobacteria for the prevention and treatment of this sort of complication. In this Lancet multi centre, randomised, double-blind, placebo-controlled, pragmatic, efficacy trial this was studied on almost 3000 patients: 10.8% diarrhoea with lactobacilli or bifidobacteria versus 10.4% diarrhoea in the placebo group. No difference!
One drug less to prescribe... Lancet 2013 Oct 12;382(9900):1249-57  In a letter to the editor of Intensive Care Medicine Soubirou et al. present the result of a study looking at the efficacy and safety of saline lock solution in maintaining short term hemodialysis catheters patency in ICU. This prospective cohort study looked at 100 double lumen hemodialysis catheters inserted in 75 patients managed with intermitted hemodialysis. At the end of each session the lumens were flushed with normal saline only. The investigators found no difference to 5 other studies using heparin or citrate. Conclusion: Heparin is not necessary in this setting, citrate is an alternative, but saline seems just as good. Soubirou JF et al. Intensive Care Med. 2014 June 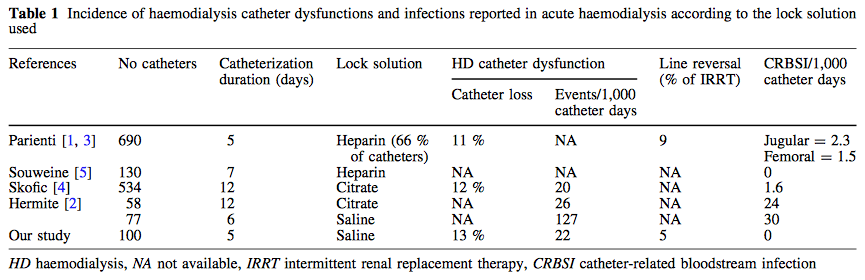 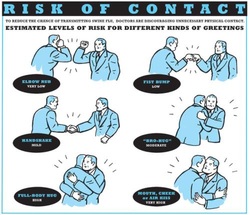 After the 2013 publication by Ghareed et al. (see BIJC post here) on fist bumps in the health care setting in order to prevent transmission of pathogens JAMA now joins in the discussion. Sklansky M et al. published a viewpoint on the banning of the handshake from the health care setting. In their paper they point out that the hands of health care workers often serve as vectors for transmission of organisms and disease. The fact is highlighted that adherence of health care providers with hand hygiene remains rather low and that handshakes have shown to be able to transmit pathogens. In their article they draw parallels between the ban of handshakes in a health care setting and the ban of smoking in public places and finally offer a variety of alternative greetings methods like: the 'hand wave' and placement of the right palm over the heart, or the Namaste gesture also practiced in yoga around the world.
This offers an interesting viewpoint worth reading indeed but I might add a few remarks and questions to this article. Apart from the fact that I still struggle to follow the link between hand shakes and smoking in public and would like to highlight following: - The link between pathogen transmission by handshakes and consecutive patient outcome is totally unclear. At this stage there is no evidence indicating that handshakes themselves impose a serious threat to patients. - Banning handshakes in hospitals might sound like a good idea, but the main problem remains unaffected. Multi-resistant bacterias are the logical result of inappropriate prescription and usage of antibiotics. It certainly is advisable to prevent the spread of these pathogens but it would be better to prevent their man made evolution. - Physical contact with patients in the ICU is an essential part in patient care (e.g. nursing or medical examination) and socialising might be even more important when you're unwell. Of course contact isolation has been found to help prevent the retransmission of pathogens. We tend to forget though that all these measures at the same time might have other unintended consequences. From 1999 to 2003 three articles showed that patients in contact isolation got half as many visits from health care providers resulting in 20% less contact time (Morgan DJ et al. Infect Control Hosp Epidemiol. 2013;34(1):69-73). Remarkably, similar effects were found also a decade later. Evidence has continued to accumulate that patients on contact precautions may experience worse outcomes, including more delirium, more depression, worse discharge instructions, and less smoking cessation counselling. Withholding a handshake sounds simple but might actually further contribute to patient's isolation and there is also some research out there actually showing on how important this gesture actually might be (Dolcos S et al. J Cogn Neurosci 2012 Dec;24(12):2292-305). The first sentence of the Conclusion by Sklansky et al. reads as follows: 'Banning the handshake from the health care environment may require further study to confirm and better describe the link between handshake-related transmission of pathogens and disease.'... I couldn't agree more! I think we might have to be very careful on already starting to talk about 'hand shake free zones' as long as there are so many unanswered questions. Many things have been done in the past to prevent infections and finally have been proven to be completely inutile (e.g. changing peripheral lines after three days, read post here). Maybe we she focus more on avoiding overprescribing antibiotics instead. What do you think...? Sklansky et al. JAMA. Published online May 15, 2014. doi:10.1001/jama.2014.4675 The picture displayed above is take from the New York Times  A situation often encountered in hospitals... also in Ireland. You have to urgently review a patient on the ward but are stuck in theatre. Of course you would like to get changed first (as hospital policy asks you to) but there are no scrubs available anymore or there are no white coats to cover your scrubs, or ... so you end up going to the ward in your scrubs... as a walking threat to patients?
Apart form the fact that changing your clothes might be appropriate to do there is this recent article of Hee at al. in Anaesthesia giving you a little chance for forgiveness. Although small in numbers these researches found no evidence that visits to ward or office significantly increase bacterial contamination of scrub suits. Hee HI et al. Anaesthesia April 18 2014 Picture above taken from the US series 'Scrubs' 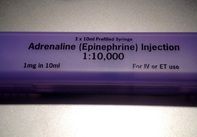 Guidelines on advanced cardiopulmonary resuscitation around the world, including the ACLS guidelines, are based on four important concepts: mechanical resuscitation (CPR), defibrillation, airway management and also application of vasoactive drugs. The application of these drugs is intended to improve hemodynamics and the heart's responsiveness to defibrillation.
What some of us might not be aware of though, but has already been mentioned by the '2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations' and the 'European Resuscitation Council Guidelines' in 2010: There is actually no definitive evidence that the application of these drugs provides any long-term benefit for these patients. While vasopressors are intended to improve coronary and cerebral perfusion and therefore successful defibrillation and neurological outcome, there is actually some concern (animal and registry studies) that this might actually decrease microcirculation and cerebral blood flow as well as increase myocardial oxygen consumption and cause post-defibrillation ventricular arrhythmias. Also the use of anti-arrhythmic drugs as well as their combination with vasopressors lacks evidence of any impact on survival. Another interesting fact is that we have no idea about ideal dosage or optimal timing of these drugs... should they be given continuously? This and many more questions and facts are discussed in an interesting review article by Sunde and Olasveengen in Current Opinion in Critical Care. They conclude that there is no evidence to support any specific drugs during cardiac arrest and that healthcare systems should not prioritise implementation of unproven drugs before good quality of care can be documented. Are we heading towards an era of drug-free resuscitation? Sunde K et al. Curr Opin Crit Care. 2014 April 16 Article accessible here  Most of us being trained as anaesthetists in the last couple of years have learnt to perform a rapid sequence induction (RSI) including the application of cricoid pressure (aka the Sellick manoeuvre) in order to prevent aspiration of gastric content.
Over the last couple of years though this manoeuvre has been seriously questioned as scientific evidence is lacking and there are concerns that cricoid pressure might actually be potentially harmful. A lot has been written on this topic so far and some great reviews can be found easily on the internet thanks to the concept of Open Free Access Meducation (FOAMed, see below). Still I would like to add some thoughts on to this discussion and maybe mention one or two more interesting facts. Cricoid pressure was actually first described by Sellick in the Lancet in 1961 as a preliminary report and basically represented an un-controlled case study in which no or only insufficient information on the studies patient population was provided. There was no standardisation of the force for cricoid pressure as of the medications used for induction. There was also no information on the quality of laryngoscopy and intubation. Steinmann and Priebe (abstract in english) have exactly analysed this publication and found some relevant methodological shortcomings. It is therefore remarkable that this publication led to an anaesthetic dogma practised all over the world. As mentioned in the European Resuscitation Council Guidelines of 2005, studies in anaesthetised patients show that cricoid pressure impairs ventilation in many patients, increases peak inspiratory pressures and causes complete obstruction in up to 50% of patients depending on the amount of pressure applied (Petito, Lawes, Hartsilver, Allman, Hocking, Mac, Ho, Shorten). The incidence of a difficult intubation is significantly higher in preclinical emergency situations than in an elective theatre environment (Timmermann A et al. Resuscitation 2007;70(2):179-185). It is therefore possible, that cricoid pressure itself actually is one of the reasons why unexperienced emergency physicians experience additional difficulties when intubating 'in the field'. One concern often mentioned is the fear that non-adherence to current guidelines by not applying cricoid pressure might have adverse legal implications. But what do current guidelines actually say? Priebe et al. partially looked at this in 2012. Several guidelines indeed still recommend cricoid pressure, sometimes even with less force in the awake patient. But some guidelines have started to implement current evidence. The 2010 Clnical Practice Guidelines on General Anaesthesia for Emergency Situations by the Scandinavian Society of Anaesthesiology and Intensive Care Medicine state following: (i) The use of CP cannot be recommended on the basis of scientific evidence (recommendation E, supported by non-randomized, historic controls, case series, uncontrolled studies and expert opinion) (ii) The use of CP is therefore not considered mandatory but can be used on individual judgement (recommendation E). (iii) If facemask ventilation becomes necessary, CP can be recommended because it may reduce the risk of causing inflation of the stomach (recommendation D, supported by non-randomized, contemporaneous controls) The 2005 European Resuscitation Council Guidelines (page 1322, pdf here) puts it this way: - The routine use of cricoid pressure in cardiac arrest is not recommended. - Studies in anaesthetised patients show that cricoid pressure impairs ventilation in many patients, increases peak inspiratory pressures and causes complete obstruction in up to 50% of patients depending on the amount of cricoid pressure (in the range of recommended effective pressure) that is applied. Still though it has to be mentioned that the Difficult Airwas Society (DAS) continues to recommend cricoid pressure for RSI on it's website. The current recommendation though seems to date back to 2004 and the question is mentioned on their website whether any pressure should be applied before loss of consciousness. Also the Association of Anaesthetists in Great Britain and Ireland recommends cricoid pressure in their AAGBI Safety Guidelines of 2009 on pre-hospital anaesthesia. It is also mentioned that 'badly applied cricoid pressure is a cause of a poor view at laryngoscopy. It may need to be adjusted or released to facilitate intubation or ventilation'. While the discussion on this issue in adults will continue the dogma of cricoid pressure might soon fall in paediatric patients as Neuhaus D et al. published a Swiss trial in 2013 where they could show that a controlled rapid sequence induction without cricoid pressure is actually safe. Further research is on its way: Trethrewy E et al. Trials. 2012 Feb 16;13:17. Until then it seems as if we are faced with guidelines mostly still in favour for cricoid pressure and evidence based medicine, which is rather discouraging us of further performing this procedure. It is good practice to constantly question current guidelines and further improve them for the patient's sake. Indeed you have to ask yourself on how far you want to stick to current guidelines for legal reasons or if you change your practice according to emerging evidence. Some of the hospitals I worked at in Switzerland have stopped performing cricoid pressure for RSI some years ago and haven't encountered any worsening in their patient outcomes. Taking into account that most RSI in the ICU resemble emergency intubations out of hospital rather than the controlled environment of a theatre I feel there are good reasons to start re-evaluating and possibly change current guidelines. Other very interesting resources of information can be found here (FOAMed): - lifeinthefastlane.com on cricoid pressure - resus.me on cricoid pressure - Update 02/05/14: Minh Le Cong published a statement of the NAP 4 investigators on his blog website: statement from NAP 4 (on prehospitalmed.com) ... The discussion goes on!  Many intensive care units try to avoid extubations at nighttime due to the fear of potentially fatal complications and possibly higher reintubation rates. However, it might actually be favourable to extubate patients as soon as possible, as this might have a positive impact on ventilation related complications and patient's length of stay. Interestingly nobody has ever looked at this special topic so far.
Tischenkel BR et al. have now looked at this topic in a retrospective cohort study of two hospitals in the state of New York. In this paper, published in the Journal of Intensive Care Medicine this month, they looked at a total of 2240 patients which were extubated in intensive care units over the period of almost 2 years. As a result they could show that nighttime extubations did not have a higher likelihood of reintubation, length of stay or mortality compared to those during the day. They conclude that patients should be extubated as soon as they meet parameters in order to potentially decrease complications of mechanical ventilation. These data, they say, do not support delaying extubations until daytime. I fully agree... as long as there is somebody in the unit able to deal with potentially deleterious complications! Tischenkel BR et al. J Intensive Care Med April 24, 2014 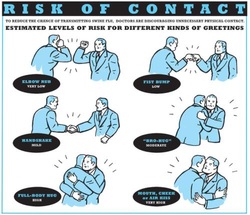 Some studies are fascinating and disconcerting at the same time... but at least they’re good for a smile!
In this paper by Ghareeb et al. the authors addressed the question whether a handshake or a fist bump is more effective in preventing or reducing pathogen transmission in the setting of a hospital, where most of us work of course. Unsurprisingly they found that using the fist bump instead of handshakes made skin contact 2.7 times shorter and this reduced spread of bacteria. They concluded that the fist bump is an effective alternative to the handshake in the hospital setting and that bumping might lead to decreased transmission of bacteria and improved health and safety of patients and health care workers alike. So shall we all start bumping around the hospital? We performed an observational study in our medium sized ICU in Galway (without approval of any committee and of course without any statistical evidence to be presented, actually just out of interest and for fun). We might also mention beforehand that working atmosphere in our unit is very good and nurses and doctors work very closely together. Interestingly, neither nursing staff nor doctors shake hands when they meet and greet each other in the ICU. The only occasions handshakes were observed are when relatives are met for a discussion or a representative of some company comes in for a visit. In regards of the study mentioned above I have some serious concerns: I wonder how many health care professionals out there would welcome a family fist bumping that has come in to discuss an end-of-life issue for instance. Also when representing the unit towards someone outside of hospital a fist bump carries some substantial risk of giving a very unprofessional impression... at least in Europe! And in very few occasions also a warm hug will be irreplaceable by some awkward bump. Social behavior is also a way on communicating... and anyhow, who pays for such studies? Ghareeb PA et al. J Hosp Infect. 2013 Dec;85(4):321-3 Picture displayed above is taken from the New York Times  JAMA just published another interesting puzzle piece on the topic of post arrest cooling. In this interesting, randomized trial, the authors addressed the question wether prehospital cooling aiming for 34°C improves outcomes after resuscitation from cardiac arrest in patients with ventricular fibrillation (VF) and non-VF. A total of 1359 patients were enrolled within 5 years. Primary outcomes were survival at hospital discharge and neurological status at discharge.
In regards of primary outcomes no differences were found between the intervention and control group. Also when looking at patients who awakened from coma or died without awakening again no significant differences between the intervention and control group were found. Also length of stay, access to early coronary angiography and reduction in level or withdrawal of life support did not differ. When looking at patient safety issues though the investigators noted a higher incidence of rearrest during transport to the hospital. The intervention group (cooled out of hospital) also showed significantly lower oxygenation on arrival, increased pulmonary edema on the first chest x-ray and a greater use of diuretics during the first 12 hours after admission. During further hospitalization though the number of days ventilated, the incidence of re-intubation and the use of antibiotics did not differ. The study results don’t support the practice of out-of-hospital cooling but show some worrying implications for patients safety. Cobb LA et al. JAMA. 2013;311(1):45-52 Open access on JAMA Network Reader (Need for sign up) Recent BIJC blog on Targeted Temperature Management Trial: Targeted Temperature Management Trial: Is it Time to Stop Cooling Patients after Cardiac Arrest?  As published in the New England Journal the ALBIOS trial has already received a lot of attention and was also one of the hot topics at the ISICEM in Brussels last week. So what’s the story.
First there is the original article published in the recent NEJM. Gattinoni et al. have looked into the potential advantages in giving 20% albumin and cristalloid solutions to hypoalbuminic patients with severe sepsis compared to cristalloid solutions only. In the albumin group they aimed for a serum albumin concentration of 30g/L (a number hardly ever seen in any ICU patient) until discharge from the ICU or 28 days after randomization. 1818 patients were included and to make things short: The trial found no difference in 28-day mortality (primary outcome), 90-day mortality (secondary outcome), or any other relevant clinical endpoint (number of patients with organ dysfunction, degree of dysfunction, length of stay in ICU and the hospital). So far for the original article. But now there is also this wonder-some supplementary appendix where the group has performed an unplanned subgroup analysis in septic shock patients only where a significant difference in the 90-day mortality was found - in favor for albumin. Indeed there is a lower number of deaths in the albumin group, but not in the p value when adjusted for clinically relevant variables. It might also be interesting to note that the 90-day mortality was a secondary endpoint and no subgroup analysis was performed of 28-day mortality among patients with septic shock. My personal view on this topic is that the original article and the supplemental appendix provide no good reason to favor albumin in the treatment of septic patients in general. The evidence provided to support the application of hypertonic albumin in septic shock patient is also not very convincing. In regards of the SAFE study from 2004 the use of albumin will remain controversial and it will be interesting to see further trials upcoming in this field. It is also worthwhile remembering that albumin remains reasonably expensive and as Prof. Takala, Bern Switzerland, mentioned in Brussels last week: the money saved on avoiding unnecessary albumin infusions might be better invested in other ICU resourced proven to improve patient outcome. Comments? Gattinoni L et al. N Engl J Med March 18, 2014 Gattinoni L et al. N Engl J Med March 18 2014: Supplemental Appendix SAFE study. N Engl J Med 2004; 350:2247-2256 |
Search
|

 RSS Feed
RSS Feed


