 Platelets are used in critical to either prevent or treat bleeding. The problem is that despite all the research and studies we still don't know that much on the best way to clinically use platelets... and they are tricky indeed:
- Platelets must be stored at room temperature - Because of the risk of bacterial growth the shelf life of platelet units is only 5 days - Maintaining a constant pool of platelets for clinical work is extremely difficult and resource-intensive - Transfusion related risks are notable (e.g. febrile reaction 1/14, allergic reactions 1/50, bacterial sepsis 1/75'000) When it comes to their usage intensivists often have a different approach than haematologists and guidelines mostly vary from hospital to hospital, from country to country. However, instead of searching all the literature yourself you might consider reading the article by Kaufman RM et al. published just this month in the Annals of Internal Medicine. A panel of 21 specialists, covering almost all areas of medicine involved in handling platelets, performed a systematic review by looking up publications from 1900 to 2013. From 1024 identified studies, 17 RCTs and 53 observational studies were included in the review. The result of their work are guidelines on the use of platelets including their grade of recommendation. Short: - Platelets should be transfused prophylactically to reduce the risk for spontaneous bleeding in hospitalized adult patients with therapy-induced hypo proliferative thrombocytopenia < 10 x 109 cells/L (Grade: strong recommendation; moderate-quality evidence) - Platelets should be transfused prophylactically for patients having elective central venous catheter placement with a platelet count less than 20 × 109 cells/L (Grade: weak recommendation; low-quality evidence) - Prophylactic platelet transfusion is recommended for patients having elective diagnostic lumbar puncture with a platelet count less than 50 × 109 cells/L (Grade: weak recommendation; very low-quality evidence) - Prophylactic platelet transfusion is recommended for patients having major elective nonneuraxial surgery with a platelet count less than 50 × 109 cells/L (Grade: weak recommendation; very low-quality evidence) - Routine prophylactic platelet transfusion for patients who are nonthrombocytopenic and have cardiac surgery with cardiopulmonary bypass (CPB) is NOT recommended. Platelet transfusion for patients having CPB who exhibit perioperative bleeding with thrombocytopenia and/or evidence of platelet dysfunction is NOT recommended (Grade: weak recommendation; very low-quality evidence) - Recommendations for or against platelet transfusion for patients receiving antiplatelet therapy who have intracranial hemorrhage (traumatic or spontaneous) cannot be made (Grade: uncertain recommendation; very low-quality evidence) It is remarkable to see that after a century of intense research we are left with some moderate-quality evidence and lots of low quality evidence and therefore weak recommendations. I guess guidelines will continue to vary from doctor to doctor, hospital to hospital... country to country. Kaufman RM et al. Ann Intern Med, Nov 11, 2014: Open access article  Thoracocentesis is a procedure often used to further determine pleural effusions. This commonly performed procedure may lead to complications including the development of a pneumothorax. Wilcox et al. performed a systematic review in JAMA of current literature to answer following two questions: 1. What are the most accurate diagnostic indicators to diagnose an exsudate? and 2. What are the most common adverse side effects and factors affecting them?
48 studies were included to answer the first question, while 37 studies were used to approach question number 2. In conclusion: - Light's criteria, pleural fluid cholesterol (<55 mg/dl) and pleural fluid LDH (>200 U/L) levels, and the pleural fluid cholesterol to serum cholesterol ratio (> 0.3) are the best diagnostic indicators for pleural exsudates - Pneumothorax was the most common complication of thoracocetesis (incidence 6%). Chest tube placement was needed in 2% of all procedures. And most impressive: Ultrasound skin marking by a radiologist or ultrasound-guided thoracocentesis were not associated with a decrease in pneumothorax events. ... would you abandon the ultrasound? Wilcox et al. JAMA, June 18, 2014, Vol 311, No. 23  The Lancet has now published the multi-centre study (PROVHILO) which has looked at the role of positive end-expiratory pressure (PEEP) for mechanical ventilation during general anaesthesia. For that reason the PROVE network investigators have included almost 900 patients in a randomised controlled trial who were planned for open abdominal surgery. All patients were ventilated with a tidal volume (Vt) of 8ml/kg. One group received a PEEP of 12 cmH2O and recruitement maneuvres while the other group got alomst no PEEP (<2 cmH2O) and no recruitement maneuvres. Primary endpoint were pulmonary compications on day 5 postoperatively. They found no difference in pulmonary complications but significantly more introperative hypotension and use of vasoactive agents in the higher PEEP group.
So the investigators conclude that a higher level of PEEP and recruitment maneuvres do not protect against postoperative pulmonary complications. They actually advise to use low tidal volumes and very low PEEP for intraoperative ventilation. The multicenter study is well designed and performed but some questions remain: Why is PEEP never adjusted to weight? One striking feature is that we all use tidal volumes according to the patients body weight, but interestingly nobody seems to use this adjustement for weight when it comes to PEEP. Using a PEEP of 12 in a small and slim 50kg patient has a different impact compared to a massively obese patient. Is 12 cmH2O too high? A PEEP of 12 can be considered generally high and is not used by most anaesthetists in their daily practice anyway. There was no third arm using intermediate levels of PEEP to answer the question on how these patient might have performed. Why did other trial find differing conclusions? The aspect of different levels of PEEP is interesting as previous studies actually were able to show improved outcome with 'protective' mechanical ventilation. The IMPROVE trial in the NEJM from Augut 2013 compared patients for abdominal surgery ventilated with Vt of 10-12ml/kg and 0 cmH2O of PEEP to patients ventilated with Vt of 6-8ml/kg and 6-10 cmH2O of PEEP. In this multicenter, double blind trial with 400 patients improved outcome and reduced health care utilazation were found in the group 'protectively' ventilated. In june 2013 Anaesthesiology published a prospective randomized small trial with 56 patients undergoing open abdominal surgery for more than 2 hours. This time they compared Vt of 9ml/kg and O PEEP to Vt of 7ml/kg and 10 PEEP. This time 'protective' ventilation with PEEP improved respiratory function but did not affect length of hospital stay. Taking these fact into account I think we remain with following conclusions: - The PROVHILO trial is not reason enough to abandon PEEP for anaesthetic ventilation in theatre - Instead we might have to consider adjusting PEEP to the patients clinical condition (e.g. weight) - There is no evidence currently to recommend routine recruitment maneuvers in theatre The Prove Network Investigators, The Lancet, Early Online Publication, 1 June 2014 Early Systematic Coronary Angiography in All Out-Of-Hospital Cardiac Arrests Seems Reasonable9/6/2014
 The most recent guidelines of the European Resuscitation Council and the American Heart Association recommend that resuscitated patients of presumed cardiac cause should undergo immediate coronary angiography with subsequent PCI if indicated, regardless of clinical symptoms and/or ECG criteria. However, this approach is discussed controversially as we don't know if there is any benefit on performing an angiography in every out-of-hospital cardiac arrest (OHCA). Additionally such an approach might be associated with quite some logistical and organisational problems for certain institutions.
In this noteworthy and open access review article Geri et al. discuss current literature and state that there are no randomised studies looking at acute coronary angiography in OHCA patients. A large number of observational studies though supports feasibility and a possible survival benefit of an early invasive approach. They conclude that even in the absence of large randomised studies, it is probable that an early coronary revascularization is associated with a significant clinical benefit in OHCA survivors. Providing the patient had no other obvious reason for OHCA (sepsis, haemorrhage, metabolic disorder etc.) current literature strongly encourages performing a systematic coronary angiography in all OHCA patients. Geri G et al., Current Opinion in Critical Care, June 2014, Vol 20, Issue 3 (Open Access)  In the most recent edition of 'Continuing Education in Anaesthesia, Critical Care and Pain' there is a very good overview article on rapid sequence induction (RSI) and its place in modern anaesthesia. Wallace and McGuire also critically look at cricoid pressure (CP) as a part of classical RSI. In their publication they state that "there have been no prospective randomized clinical studies performed to prove the clinical hypothesis and the level of evidence to support the use of cricoid pressure is poor (Level 5)". Level 5 corresponds to 'Expert Opinion' (see table below). They also mention that aspiration has occured despite CP, that CP is often poorly performed, that it may hinder bag-valve mask ventilation as well as LMA insertion and that is may worsen laryngoscopy. It's mentioned that "Critically, it has also been shown to potentially obstruct the upper airway and reduce time to desaturation". 'This is nothing new' you might say. Why am I mentioning this? Well, the remarkable thing about this article is the fact that it was published in a Journal that is a joint venture of the British Journal of Anaesthesia BJA and The Royal College of Anaesthetists in collaboration with the Intensive Care Society and Pain Society. Considering the fact that The NAP4 guidelines continue to support its use as part of an RSI and as such, it is still considered a standard of care in the UK and therefore also Ireland, this publication might indicate some change in mind... or not? The authors summarize: Application of cricoid pressure is advisable — unless it obscures the view at laryngoscopy or interferes with manual ventilation or supraglottic airway device placement. I personally still would want to know what exactly makes a 'Level 5' medical intervention 'advisable' especially in regards of all the possible problems and complications associated with it. Wallace et al., Continuing Education in Anaesthesia, Critical Care & Pain, Volume 14(3), June 2014, p 130–135 Read our previous BIJC post: Cricoid Pressure for RSI in the ICU: Time to Let Go? (Updated) 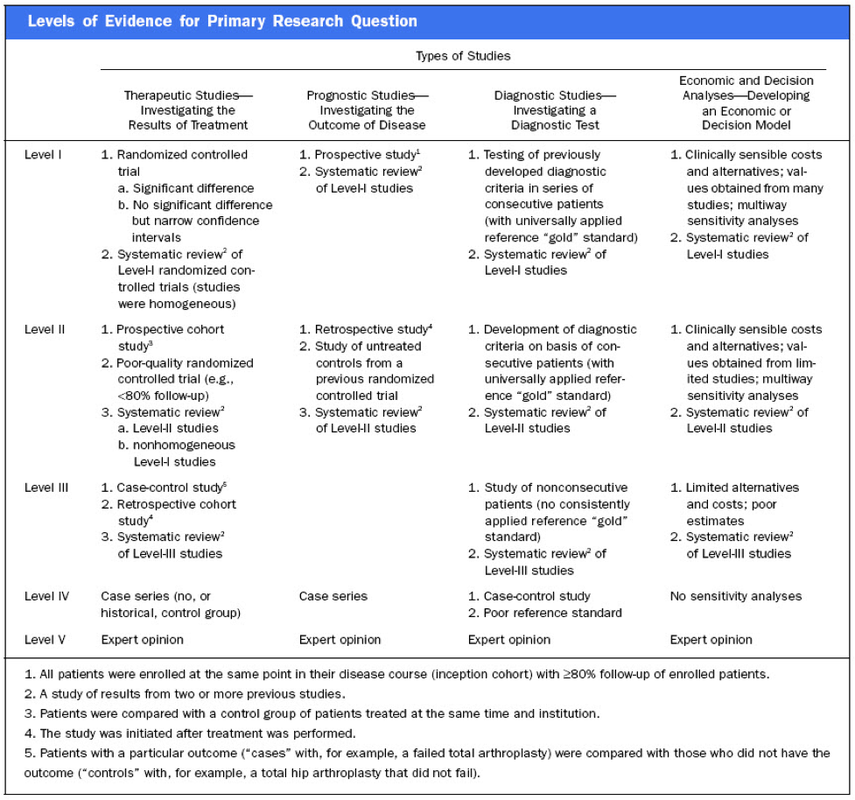  In a letter to the editor of Intensive Care Medicine Soubirou et al. present the result of a study looking at the efficacy and safety of saline lock solution in maintaining short term hemodialysis catheters patency in ICU. This prospective cohort study looked at 100 double lumen hemodialysis catheters inserted in 75 patients managed with intermitted hemodialysis. At the end of each session the lumens were flushed with normal saline only. The investigators found no difference to 5 other studies using heparin or citrate. Conclusion: Heparin is not necessary in this setting, citrate is an alternative, but saline seems just as good. Soubirou JF et al. Intensive Care Med. 2014 June 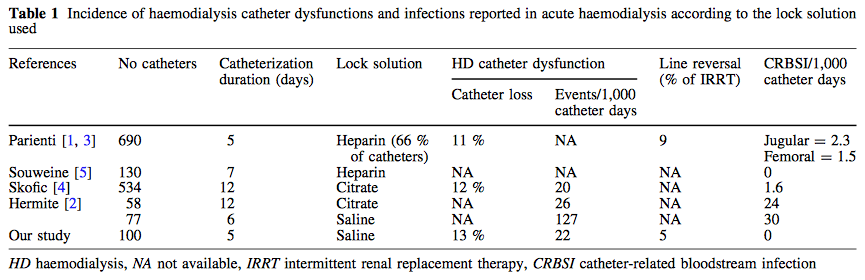  A situation often encountered in hospitals... also in Ireland. You have to urgently review a patient on the ward but are stuck in theatre. Of course you would like to get changed first (as hospital policy asks you to) but there are no scrubs available anymore or there are no white coats to cover your scrubs, or ... so you end up going to the ward in your scrubs... as a walking threat to patients?
Apart form the fact that changing your clothes might be appropriate to do there is this recent article of Hee at al. in Anaesthesia giving you a little chance for forgiveness. Although small in numbers these researches found no evidence that visits to ward or office significantly increase bacterial contamination of scrub suits. Hee HI et al. Anaesthesia April 18 2014 Picture above taken from the US series 'Scrubs'  Most of us being trained as anaesthetists in the last couple of years have learnt to perform a rapid sequence induction (RSI) including the application of cricoid pressure (aka the Sellick manoeuvre) in order to prevent aspiration of gastric content.
Over the last couple of years though this manoeuvre has been seriously questioned as scientific evidence is lacking and there are concerns that cricoid pressure might actually be potentially harmful. A lot has been written on this topic so far and some great reviews can be found easily on the internet thanks to the concept of Open Free Access Meducation (FOAMed, see below). Still I would like to add some thoughts on to this discussion and maybe mention one or two more interesting facts. Cricoid pressure was actually first described by Sellick in the Lancet in 1961 as a preliminary report and basically represented an un-controlled case study in which no or only insufficient information on the studies patient population was provided. There was no standardisation of the force for cricoid pressure as of the medications used for induction. There was also no information on the quality of laryngoscopy and intubation. Steinmann and Priebe (abstract in english) have exactly analysed this publication and found some relevant methodological shortcomings. It is therefore remarkable that this publication led to an anaesthetic dogma practised all over the world. As mentioned in the European Resuscitation Council Guidelines of 2005, studies in anaesthetised patients show that cricoid pressure impairs ventilation in many patients, increases peak inspiratory pressures and causes complete obstruction in up to 50% of patients depending on the amount of pressure applied (Petito, Lawes, Hartsilver, Allman, Hocking, Mac, Ho, Shorten). The incidence of a difficult intubation is significantly higher in preclinical emergency situations than in an elective theatre environment (Timmermann A et al. Resuscitation 2007;70(2):179-185). It is therefore possible, that cricoid pressure itself actually is one of the reasons why unexperienced emergency physicians experience additional difficulties when intubating 'in the field'. One concern often mentioned is the fear that non-adherence to current guidelines by not applying cricoid pressure might have adverse legal implications. But what do current guidelines actually say? Priebe et al. partially looked at this in 2012. Several guidelines indeed still recommend cricoid pressure, sometimes even with less force in the awake patient. But some guidelines have started to implement current evidence. The 2010 Clnical Practice Guidelines on General Anaesthesia for Emergency Situations by the Scandinavian Society of Anaesthesiology and Intensive Care Medicine state following: (i) The use of CP cannot be recommended on the basis of scientific evidence (recommendation E, supported by non-randomized, historic controls, case series, uncontrolled studies and expert opinion) (ii) The use of CP is therefore not considered mandatory but can be used on individual judgement (recommendation E). (iii) If facemask ventilation becomes necessary, CP can be recommended because it may reduce the risk of causing inflation of the stomach (recommendation D, supported by non-randomized, contemporaneous controls) The 2005 European Resuscitation Council Guidelines (page 1322, pdf here) puts it this way: - The routine use of cricoid pressure in cardiac arrest is not recommended. - Studies in anaesthetised patients show that cricoid pressure impairs ventilation in many patients, increases peak inspiratory pressures and causes complete obstruction in up to 50% of patients depending on the amount of cricoid pressure (in the range of recommended effective pressure) that is applied. Still though it has to be mentioned that the Difficult Airwas Society (DAS) continues to recommend cricoid pressure for RSI on it's website. The current recommendation though seems to date back to 2004 and the question is mentioned on their website whether any pressure should be applied before loss of consciousness. Also the Association of Anaesthetists in Great Britain and Ireland recommends cricoid pressure in their AAGBI Safety Guidelines of 2009 on pre-hospital anaesthesia. It is also mentioned that 'badly applied cricoid pressure is a cause of a poor view at laryngoscopy. It may need to be adjusted or released to facilitate intubation or ventilation'. While the discussion on this issue in adults will continue the dogma of cricoid pressure might soon fall in paediatric patients as Neuhaus D et al. published a Swiss trial in 2013 where they could show that a controlled rapid sequence induction without cricoid pressure is actually safe. Further research is on its way: Trethrewy E et al. Trials. 2012 Feb 16;13:17. Until then it seems as if we are faced with guidelines mostly still in favour for cricoid pressure and evidence based medicine, which is rather discouraging us of further performing this procedure. It is good practice to constantly question current guidelines and further improve them for the patient's sake. Indeed you have to ask yourself on how far you want to stick to current guidelines for legal reasons or if you change your practice according to emerging evidence. Some of the hospitals I worked at in Switzerland have stopped performing cricoid pressure for RSI some years ago and haven't encountered any worsening in their patient outcomes. Taking into account that most RSI in the ICU resemble emergency intubations out of hospital rather than the controlled environment of a theatre I feel there are good reasons to start re-evaluating and possibly change current guidelines. Other very interesting resources of information can be found here (FOAMed): - lifeinthefastlane.com on cricoid pressure - resus.me on cricoid pressure - Update 02/05/14: Minh Le Cong published a statement of the NAP 4 investigators on his blog website: statement from NAP 4 (on prehospitalmed.com) ... The discussion goes on!  Many intensive care units try to avoid extubations at nighttime due to the fear of potentially fatal complications and possibly higher reintubation rates. However, it might actually be favourable to extubate patients as soon as possible, as this might have a positive impact on ventilation related complications and patient's length of stay. Interestingly nobody has ever looked at this special topic so far.
Tischenkel BR et al. have now looked at this topic in a retrospective cohort study of two hospitals in the state of New York. In this paper, published in the Journal of Intensive Care Medicine this month, they looked at a total of 2240 patients which were extubated in intensive care units over the period of almost 2 years. As a result they could show that nighttime extubations did not have a higher likelihood of reintubation, length of stay or mortality compared to those during the day. They conclude that patients should be extubated as soon as they meet parameters in order to potentially decrease complications of mechanical ventilation. These data, they say, do not support delaying extubations until daytime. I fully agree... as long as there is somebody in the unit able to deal with potentially deleterious complications! Tischenkel BR et al. J Intensive Care Med April 24, 2014  Do you use text messages (sms) in your ICU? Of course you do... we all do! It seem sometimes a little worrying to see how text messaging has secretly creeped into clinical life in hospitals. Apart from simply talking to each other on the phone clinicians increasingly use text messaging to exchange patient informations.
Recent revelations by whistleblowers like Edward Snowden have made us very aware of the fact that exchanged text messages can be easily intercepted and therefore read by a third party. The worst case scenario would be the publication of confident patient information. The chance, that patient information will leak in that sort of way is not very big, but 'Medical Identity Theft' happens and now slowly starts to find it's way into medical publications. The World Privacy Forum estimates, that 250'000 to 500'000 people have already been victimised by this sort of crime since 1995. So this kind of threat should be taken seriously. The Society of Critical Care Medicine has just recently published an article on this issue that nicely shows the different challenges we encounter by using all different sorts of mobile devices. Medical societies have not yet specifically given any recommendations on this topic, but it is clear that all private health information must be protected against any threat on confidentiality. The Joint Commission, an institution involved in the accreditation of medical institutions all around the world, gets very specific on the use of text messages: “Physicians who need to quickly communicate time-sensitive information about their patients should no longer use text messages.” So what can we do in clinical practice? One option is to start using encrypted services (e.g. Threema). But then again technical issues between different sort of mobile devices might be problematic. And different people might use different applications. The question remains if simple text messages can be considered safe by simply using de-identified information. What do you do in your hospital...? Christine C. Toevs, SCCM on Communication, February 2014  It has been almost for 40 years that the positive effect of prone positioning in ARDS patients was recognised. But even up to 2012 no benefit on mortality could be found in several studies and also the duration of prone positioning was not found to make any difference. In June 2013 Guerin et al. published the PROSEVA trial which indeed showed some amazing results. It is the 5th biggest trial of it's kind and finally was able to actually now show a dramatic reduction in mortality: the 28 day mortality was 32.8% in the supine group (229 patients), compared to only 16% in the prone group (237 patients). This benefit in outcome persisted also after 90 days... a miracle? Most probably these results reflect the very strict adherence to the guidelines of ARDSnet in regards of paralysation and use of very low tidal volumes. One thing that has to be mentioned is the high number of patients with ARDS which have excluded from the trial for several reasons. So should we now follow this study and prone more aggressively? One answer might be the just recently published meta-analysis by Lee at al. in Critical Care Medicine. This paper looked at a total of 11 randomised controlled trials and therefore takes all recent publications into account. The authors come to the conclusion that prone positioning indeed does reduce mortality significantly and were marked in the subgroup where the duration of prone positioning was more than 10 hours. This is the first time somebody actually comments on the length of prone positioning in terms of benefit for the patient. As always though there are also adverse effects of this therapy as prone positioning was significantly associated with pressure sores and maybe most importantly major airway problems. Overall, the concept of prone positioning in severe ARDS seems to be well established and should be implemented in the clinical procedures of every intensive care unit. This is particularly true for regions where quick access to extra corporal CO2 removal or oxygenation devices is difficult. Guerin C et al. N Engl J Med. 2013 Jun 6;368(23):2159-68. Lee JM et al. Crit Care Med. 2014 May;42(5):1252-62. Ferguson et al. Intensive Care Med. 2012 Oct;38(10):1573-82. A very nice and quick overview on treatment options for ARDS was presented by Ferguson et al. in Intensive Care Medicine 2012: 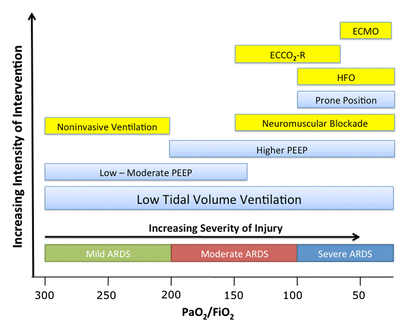
 JAMA just published another interesting puzzle piece on the topic of post arrest cooling. In this interesting, randomized trial, the authors addressed the question wether prehospital cooling aiming for 34°C improves outcomes after resuscitation from cardiac arrest in patients with ventricular fibrillation (VF) and non-VF. A total of 1359 patients were enrolled within 5 years. Primary outcomes were survival at hospital discharge and neurological status at discharge.
In regards of primary outcomes no differences were found between the intervention and control group. Also when looking at patients who awakened from coma or died without awakening again no significant differences between the intervention and control group were found. Also length of stay, access to early coronary angiography and reduction in level or withdrawal of life support did not differ. When looking at patient safety issues though the investigators noted a higher incidence of rearrest during transport to the hospital. The intervention group (cooled out of hospital) also showed significantly lower oxygenation on arrival, increased pulmonary edema on the first chest x-ray and a greater use of diuretics during the first 12 hours after admission. During further hospitalization though the number of days ventilated, the incidence of re-intubation and the use of antibiotics did not differ. The study results don’t support the practice of out-of-hospital cooling but show some worrying implications for patients safety. Cobb LA et al. JAMA. 2013;311(1):45-52 Open access on JAMA Network Reader (Need for sign up) Recent BIJC blog on Targeted Temperature Management Trial: Targeted Temperature Management Trial: Is it Time to Stop Cooling Patients after Cardiac Arrest? Targeted Temperature Management Trial: Is it Time to Stop Cooling Patients after Cardiac Arrest?6/1/2014
 In 2002 two published articles in the New England Journal of Medicine changed ICU management of out of hospital arrests profoundly. According to these two articles (cited below) the American Heart Association labeled this to be good evidence (Level1) to recommend induced hypothermia in comatose survivors of out of hospital cardia arrest caused by VF. The target temperature was recommended to be between 32-34°C and to be maintained for 12-24 hours.
And now this... Nielsen et al. present the Targeted Temperature Management Trial showing, that there is NO difference between patients cooled to 33°C and patients kept at 36°C. Is this the end of the cooling era, should we change our management? I personally think think that this trial basically adds up to our knowledge in the field of post cardiac arrest care, but not necessarily contradicts the previous two trials. We now have one trial showing that there seems to be no difference between 33°C and 36°C but we also know, that hyperthermia (pyrexia) is troublesome and associated with worse neurological outcome. So, as pronounced hypothermia (33°C) makes no difference to ‘mild’ hypothermia (36°C) and pyrexia is proven to be harmful... the question is: What is the right temperature? We seem to head towards normothermia or mild hypothermia in order to provide best management for our patients. It’s going to be interesting to see how recommendations will change in the near future. The Targeted Temperature Management Trial: Nielsen N, et al. New Engl J Med. 2013 Dec;369(23):2197-206 The 2 trials that introduced therapeutic hypothermia into ICU practice: The Hypothermia After Cardiac Arrest Study Group, Holzer at al. New Engl J Med. 2002 Feb;346(8):549-556 Bernard S.A. et al. New Engl J Med. 2002 Feb;346(8):557-563 Review article on therapeutic hypothermia for non-VF/VT cardiac arrest: Sandroni S. et al. Crit Care Med; 2013;17:215 Pyrexia and neurological outcome: Leary M. et al. Resuscitation. 2013 Aug;84(8):1056-61  Inspired by an excellent post by Dr. Pat Nelligan on AnaesthesiaWest we would like to provide even more evidence against routine change of IV catheters... just because you are told to do so for hospital policy reasons.
Brown D. et al. have provided an excellent overview article on this issue. It is clearly shown that peripheral IV catheter should be replaced as clinically indicated, rather than on a routine basis. The level of evidence here is: A. This means that this recommendation of this treatment/ procedure is effective! We add another 3 articles supporting this recommendation. We do many other things on ICU with lower levels of evidence, or even no evidence at all. So it is definitely time to change this bad habit. So Pat, I won’t do it either... full stop! Bregenzer T, et al. Arch Intern Med, January 1998; 158(2):151-6 Lee WL, et al. Am J Infect Control, 2009 Oct;37(8):683-6 Lai KK, et al. Am J Infect Control, 1998 Feb;26(1):66-70 X-rays still remain the most widely used primary investigation for query pneumothorax. In recent years, ultrasound has become increasingly popular for this question in ICU’s around the world... but what is better? This article conducted a meta-analysis including 13 studies from 2002-2012. They were able to show that pleural ultrasound is more sensitive indeed compared to chest radiography in detecting a pneumothorax. It is interesting to note, that most studies were related to trauma patients and only one was conducted by intensivists. Maybe it’s because verifying catheter positions with normal ultrasound remains challenging.
A nice tutorial can be found here: Tutorial Ultrasound for pneumothorax Saadah A, et al. Critical Care, November 2013. Provisional article, in print |
Search
|

 RSS Feed
RSS Feed


