 Clinicians are confronted every day with a growing number pacemakers (PMs), implantable cardioverter-defibrillators (ICDs) and implantable loop recorders (ILRs). Collectively these devices are sub summarised as cardiac rhythm management devices (CRMDs). Identification of these devices is simple as long a the patient can present an ID card or some other form of identification. This can become challenging especially in emergencies where such information might not be accessible, and interrogation of the pacemaker becomes a problem. Using the wrong manufacturer-specific device programmer causes a delay in diagnostic and treatment and can be relevant in these situations. Techniques to identify a CRMD are following: - Patient's ID card - Medical records - Manufacturers' patient registries (All CRMD manufacturers keep their own in-house registry of patients implanted with their devices and provide 24-hour telephone technical support - Device specific radiopaque alphanumeric codes (ANC) All these identification techniques have their problems in clinical practice, and so far no other method or algorithm was available to help out in such a dilemma. Sony Jacob et al. have therefore developed and validated the so-called Cardiac Rhythm Device Identification Algorithm using X-rays (CaRDIA-X, see below) The study participants using this algorithm showed an overall accuracy of 96.9%. This study was published in 2011 but only now caught our attention.  We have tried this algorithm on a few X-rays ourselves and came to the conclusion: Using the chart is a little challenge itself, but very helpful in most cases! Certainly worth keeping in mind! Jacob S et al. Heart Rhythm. 2011 Jun;8(6):915-22.  When filling out the form for a CT scan in you hospital you will not only have to provide clinical information about the patient but almost certainly also the latest creatinine levels. This information is required as many clinicians are worried that IV contrast media might cause iatrogenic acute kidney injury and therefore increased rates of dialysis, renal failure, and death. Despite several reports of contrast-induced nephropathies in the past, the causal relationship between IV contrast media and the development of acute kidney injury has been challenged recently (Read our previous summary HERE). 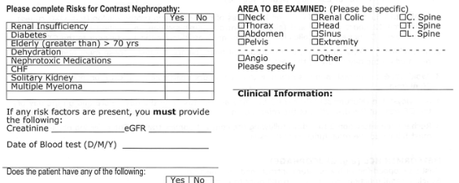
The major problem is that performing a randomized controlled trial to elucidate the true incidence of contrast-induced nephropathy is considered unethical because of the presumption that contrast media administration is a direct cause of acute kidney injury. While the discussion goes on Hinson et al. have come up with another nice piece of evidence that in emergency situations there is no reason to withhold the application of IV contrast for CT scans when required. In this single-center retrospective cohort study researchers have included a total of 17'934 patient visits to their emergency department over a period of 5 years. They analysed three patient groups that where demographically similar: contrast-enhanced CT, unenhanced CT and no CT scan performed. Patients were included when their initial serum creatinine level was between 35 umol/L and 352 umol/L. Of all CT scans, 57.2 percent were contrast-enhanced. The probability of developing acute kidney injury was 6.8 percent for patients undergoing contrast-enhanced CT, 8.9 percent for patients receiving unenhanced CT and 8.1 percent for patients not receiving CT at all. This proofs to be the largest controlled study of its kind in the emergency department and shows that: In current clinical context, contrast media administration for CT scans is NOT associated with an increased incidence of acute kidney injury. And even though a large randomised controlled trial is still missing it seems safe... To Conclude: There is no reason to withhold the use of IV contrast media in cases where contrast-enhanced CT is indicated to avoid delayed or missed diagnosis of critical disease. Hinson J et al. Annals of Emergency Medicine, 2017; DOI: 10.1016/j.annemergmed.2016.11.021 OPEN ACCESS Crit Cloud Review from 18/01/2015 Iodinated Radiocontrast Agents can cause Kidney Injury... But not as much as we thought they would!12/3/2014
 One major concern when bringing a critically ill patient for a CT scan is the potential for acute kidney injury (AKI) by applying iodinated contrast media intravenously. Post-contrast AKI carries the risk of more permanent renal failure, dialysis and even death. The authors of this review article nicely summarize current evidence on this issue and show, that the risk of AKI secondary to contrast material (particularly when administered intravenously for contrast-enhanced CT) has been exaggerated in the past by older, noncontrolled studies.
In fact, by reviewing more recent evidence they come to the conclusion that the risk is almost nonexistent in patients with normal renal function. Even in patients with pre-existing renal insufficiency the risk of secondary contrast-induced AKI is probably much smaller than traditionally assumed. Again they emphasize on the fact that volume expansion is the only preventive strategy with a convincing evidence base. Nevertheless, the benefits of a contrast-enhanced exam still will have to be balanced with the remaining risk of AKI. BioMed Research International. 2014, Article ID 859328 X-rays still remain the most widely used primary investigation for query pneumothorax. In recent years, ultrasound has become increasingly popular for this question in ICU’s around the world... but what is better? This article conducted a meta-analysis including 13 studies from 2002-2012. They were able to show that pleural ultrasound is more sensitive indeed compared to chest radiography in detecting a pneumothorax. It is interesting to note, that most studies were related to trauma patients and only one was conducted by intensivists. Maybe it’s because verifying catheter positions with normal ultrasound remains challenging.
A nice tutorial can be found here: Tutorial Ultrasound for pneumothorax Saadah A, et al. Critical Care, November 2013. Provisional article, in print |
Search
|

 RSS Feed
RSS Feed


