Mind the GAPS Study - Compression Stockings are Useless for Most Elective Surgery Patients!14/9/2020
 Cricoid pressure prevents aspirations, preoperative antibiotics avoid infections, and compression stockings protect against deep vein thrombosis. Many medical measures aim to reduce morbidity and mortality among patients, but unfortunately, the benefit of these measures is often not, or insufficiently, proven. Under certain circumstances, they may lead to additional problems or even cause harm (e.g. cricoid pressure Read Here). Time has definitely come to take a closer look at compression stockings for surgical patients. Apart from the fact that they look terrible, they are just as uncomfortable to wear and even carry certain risks in patients with peripheral vascular disease, for example. The effectiveness of compression stockings in modern practice has been questioned, but robust evidence has been lacking. This seems to change, as the long-awaited GAPS-Trial has been published and now provides further evidence on what concern patients undergoing elective surgery. 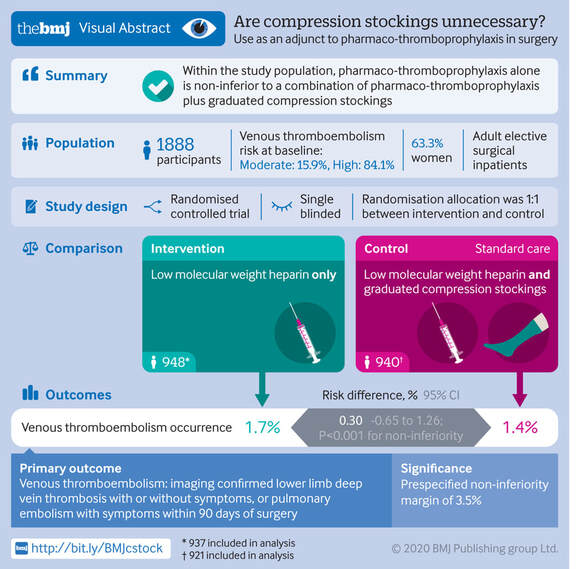 Among this population, adding compression stockings to pharmaco-thromboprophylaxis was non-superior compared to pharmaco-thromboprophylaxis alone (primary outcome). There was also no difference in the quality of life outcomes found (secondary outcome).  There is now some robust evidence to omit compression stockings in surgical patients that receive pharmacological thromboprophylaxis. Shalhou J. et al. BMJ 2020;369:m1309  The W.H.O. has repeatedly warned that antibiotic resistance is one of the biggest threats to global health today. Among all measures we can take to try and reduce this problem, merely avoiding unnecessary treatments is maybe one of the most effective. It is therefore pleasing that another piece of good evidence has been published, supporting the avoidance of antibiotics in the event of non-complicated diverticulitis (defined as non-perforated diverticulitis with a Hinchey 1a grade in computed tomography). The investigators performed a randomized, placebo-controlled, double-blind trial in which they compared 180 patients with non-complicated diverticulitis to receive either cefuroxime, metronidazole, and amoxicillin/clavulanic acid or placebo. They found No significant difference in the median time of hospital stay (primary outcome). Also, there were no significant differences between groups in adverse events, readmission to the hospital within one week, and readmission to the hospital within 30 days.  These findings complement other studies indicating that observational treatment without antibiotics can be considered appropriate in patients with uncomplicated diverticulitis.  The lastest updated surviving sepsis guidelines for COVID-19 patient recommends a high-peep strategy in the intubated, mechanically ventilated patient. As most of these patients present with moderate to severe ARDS, PEEP is used to keep lung areas open and therefor to improve oxygenation. This seems to be especially true in the classical case of ARDS, where the lung become 'wet' and 'heavy' which results in widespread atelectasis of the dependent parts of the lungs, often further complicated by pleural effusions. Classical CT appearance in the acute phase of ARDS is an opacification with an antero-posterior density gradient. Dense consolidation in the most dependent regions merges into a background of widespread ground-glass attenuation and the normal or hyperexpanded lung in the non-dependent areas (Howling SJ et al. Clin Radiol 1998;53(2):105-109). The theory behind these changes is that the increased weight of overlying lung causes compression-atelectasis posteriorly. The fact that prone positioning these patients quickly redistributes these gradients supports this theory (Desai SR et al. Anaesthesiology 1991;74(1):15-23). 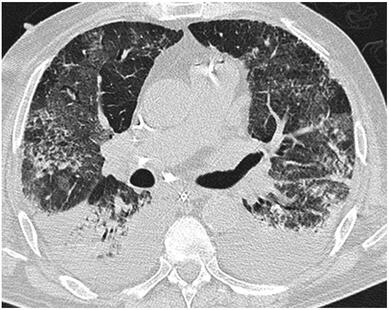 Classical ARDS finding in pneumococcal pneumonia Chest CT's in patients with COVID-19 often show ground-glass opacification with or without consolidations. These are changes often seen in viral pneumonia. Several case series suggest, that CT abnormalities seem to be mostly bilateral and tend to have a peripheral distribution, often involving the lower lobes. In contrast to the classical ARDS pleural thickening, pleural effusion and lymphadenopathy seem to be a less common finding (Shi H et al. Lancet Infect Dis 2020). 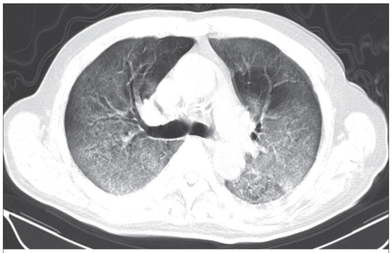 ARDS in COVID-19 patient The leading problem in COVID-19 patients with ARDS is hypoxemia, while hypercapnia does not seem to be a significant problem. Sometimes profound hypoxemia does not seem to correlate with patient symptoms at all. In regards to the images above, atelectasis might not be the predominant reason for V/Q mismatches in these patients. Observations of mechanically ventilated patients in our unit and other hospitals in Switzerland have shown, that higher PEEP levels (15cmH2O and higher) often result in significantly reduced compliance values complicating ventilation and favouring the development of pulmonary over-inflation. This observation might support the theory that patients with COVID do not represent the traditional manner of ARDS with distinctive atelectasis. Another observation that supports this theory is that COVID-19 patients often do not respond as clearly to Prone Positioning as classical ARDS patients do. More probably, V/Q mismatch seems so happen on a more microscopical level in COVID-Patients. Lung compliance is often normal on these patients and, therefore, applying high PEEP-levels does NOT add any benefit at all. Maybe the principle of less is more also applies to COVID-19 patients we treat (Gattinoni L et al. Intensive Care Medicine; 46, pages780–782(2020)) Looking at the New Surviving Sepsis Campain COVID-19 Guidelines: Given these considerations, the strategy with High PEEP-levels in general should be questioned in principle.  The International Liaison Committee on Resuscitation has published the last guidelines for advanced cardiac life support (ACLS) on resuscitation ILCOR in 2015. Usually, these statements are updated every five years, but 'Circulation' has now published an AHA (American Heart Association) focused update due to an increased number of studies looking at ACLS-specific interventions. These updates are focused on three specific areas:
No News in regards to Vasopressors and ECPR Vasopressors in Cardiac Arrest
The bottom line: Great, these recommendations are no real news and do not change current guidelines at all. Extracorporeal Cardiopulmonary Resucitation ECPR
The bottom line: ECPR is not for on the roads and remains an exception in general. Advanced Airway Management Taking recent evidence into account the updated guidelines 2019 conclude:
We Suggest: Put the Supraglottic Airway First!In regards to these updated guidelines, the necessity of optimal cardiopulmonary resuscitation (CPR) during resuscitation and practical considerations, it seems reasonable to put the supraglottic airway (SGA) to the very top of airway management! Here is why:
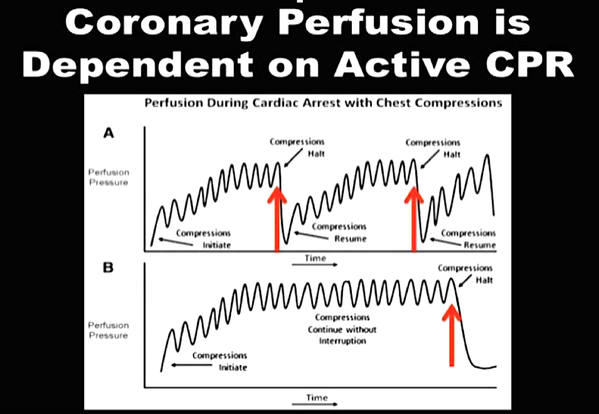 Avoiding interruptions is the key to successful CRP and therefore survival
On the other hand
It, therefore, seems plausible to put the supraglottic airway first. Not only first as a choice of airway management, but also one of the first things to do:
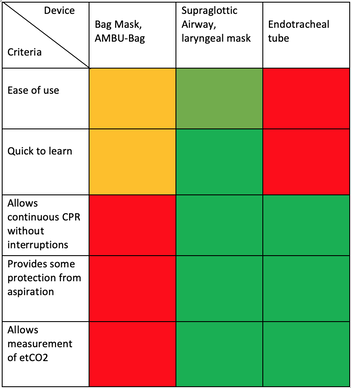 Summary of Evidence and Experience on Airway-Devices used for CRP The International Liaison Committee on Resuscitation (ILCOR) has again carried together all evidence and recently published more than 50 new ILCOR treatment recommendations and scoping reviews. You can find these documents right here: https://costr.ilcor.org This website provides an excellent systematic review of the Advanced Airway Management during Adult Cardiac Arrest, containing references to all relevant evidence available.  Based on this and given the experience from everyday clinical practice, it would be worth considering supplementing the recommendations as follows. - For resuscitation performed by health care professionals (physicians, nurses, paramedics), the use of a supraglottic airway (ideally non-inflatable) as soon as possible is recommended. 2019 AHA Focused Updated on Adult Cardiovascular Life Support  The headlines in the news 2017 were remarkable indeed: "Doctor believes he has found the cure for sepsis..." or "Doctor says improvised 'cure' for sepsis has had remarkable results". Dr. Paul Marik described his observation in an interview in 2017, where he mentions several cases of sepsis that have almost miraculously responded to the application of vitamin c (watch here: Interview on WAVY TV). He even continues, that since then they see "the same thing over and over again". This implicated that these results were reproducible. He finally stated that the current data at that stage were "impressive" and that there was enough basic science to show that it works. Vitamin C has many interesting properties that theoretically could be on benefit in sepsis. (read here: Crit☁ post on Vitamin C). Its application was already proposed for the treatment of other diseases like the common cold of Influenza. Despite some moderate positive influence observed, these results could not be reproduced in trials. While the news picked up on this story as a miracle drug, Paul Marik et al. published their results of a before-and-after single-centre, retrospective cohort study in Chest 2017. In this paper, they compared 47 patients with sepsis that received the metabolic cocktail (Vitamin C 1.5g 6-hourly, hydrocortisone 50mg 6-hourly and thiamine 200mg 12-hourly) to 47 patients which did not - notably in a non-double-blinded, non-randomized fashion. Their results showed overall hospital mortality of 8.5% with the 'cocktail' and 40.4% without its application. This publication was reason enough to launch a small war of faith about sense and nonsense of this cocktail for sepsis. The VITAMINS Trial - First FailureSince 2017 a tiny bunch of studies were published, many of them with significant limitations like a small number of patients, often not randomized-controlled and with conflicting results. Nabil Habib T, Ahmed I (2017) Early Adjuvant Intravenous Vitamin C Treatment in Septic Shock may Resolve the Vasopressor Dependence. Int J Microbiol Adv Immunol. 05(1), 77-81. Shin et al. J Clin Med. 2019 Jan; 8(1): 102. Fowler et al. JAMA. 2019 Oct 1;322(13):1261-1270. Fujii et al. have just now published the first more substantial and rigorous trial taking a closer look at the influence on vitamin c in sepsis. They performed an international, multicenter, randomized-controlled open label trial In which they enrolled 211 patients with septic shock admitted to an ICU. They compared Treatment with Vitamin C 1.5g 6-hourly IV, hydrocortisone 50mg 6-hourly IV and thiamin 200mg 12-hourly IV to Hydrocortisone 50mg 6-hourly IV only. They found No difference in time alive and time free of vasopressors (primary endpoint) and No difference 28 days or 90 days mortality (secondary endpoint) This first study on a larger scale, unfortunately, disappoints. More trials are on the way and might give a clearer picture of this topic to come to a final decision eventually. For the moment it is appropriate to state: 
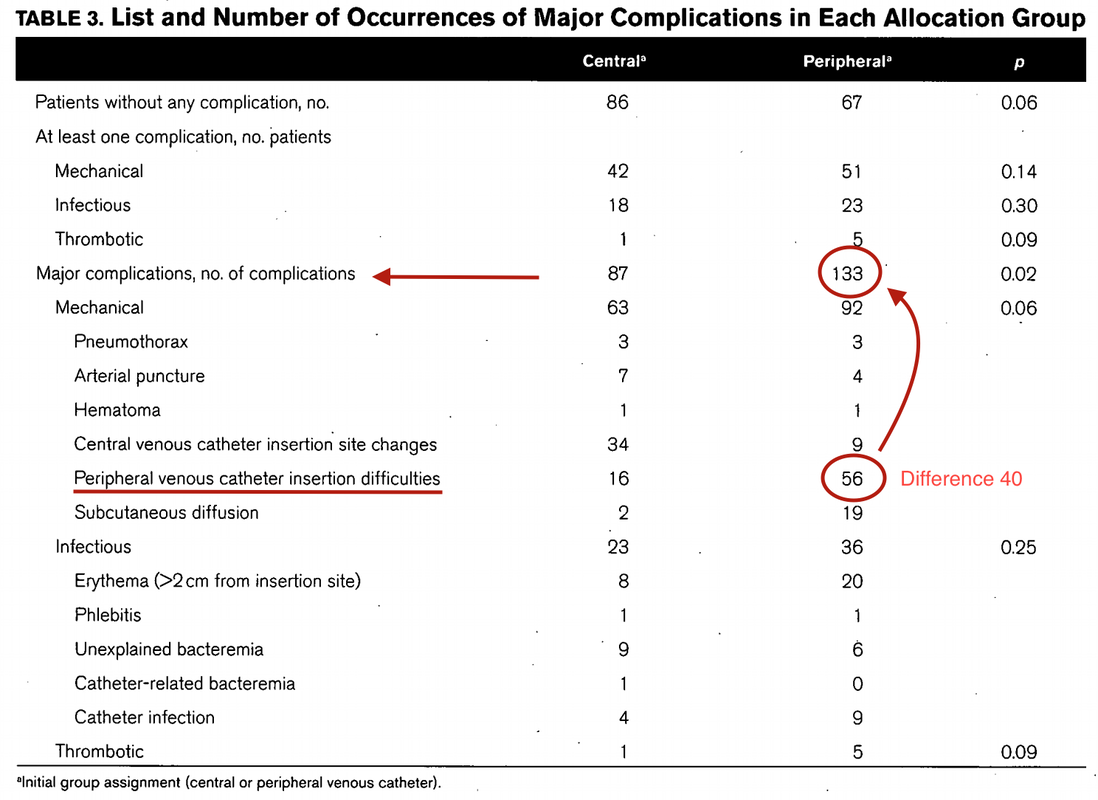
Just as a reminder: Guidelines recommend against the routine use of glucocorticoids in patients with sepsis. However, corticosteroid therapy is appropriate in patients with septic shock that is refractory to adequate fluid resuscitation and vasopressor administration. Fujii et al. JAMA. Published online January 17, 2020. doi:10.1001/jama.2019.22176  Teaching in medical school and opinions in literature are in agreement: The application of vasopressors requires central venous access. The reason for this are concerns that vasopressors given over a peripheral venous catheter (PCV) may cause phlebitis or even worse necrosis or ischemia through extravasation. While irritation of a peripheral vein is often observed with the administration of drugs like potassium or amiodarone, this usually is not the case with the application of, e.g. norepinephrine. Besides, it is essential to keep in mind that the insertion of a central venous catheter (CVC) is technically demanding and takes a certain amount of time when performed correctly. The procedure is also associated with potentially dangerous complications that might be hazardous to the patient. Therefore a fundamental question arises: Do all patients that require vasopressors need a central venous catheter? What about the peripheral access (PVC) - Any dangers there?
|




The SPICE III Trial |  |
Precisely this question was now addressed by Shehabi et al., published in the NEJM
They performed an
International (8 countries, 74 ICU's), randomised controlled, unblinded trial
In which they evaluated
4000 ICU patients that were expected to need mechanical ventilation for at least 48 hours and required sedation for safety or comfort
They compared
Patients sedated with propofol, midazolam or other agents as prescribed by the treating physician with patients receiving dexmedetomidine as a continuous infusion
(if DEX alone was insufficient, other agents could be added! In fact, 64% of patients also received propofol, 3% midazolam and 7% received both)
They found
1. No difference in 90-day mortality (primary outcome) and
2. No difference in death after 180 days, institutional dependency at 180 days, mean cognitive decline and assessment of the quality of life. Also no difference in median days free from coma to day 28 and median ventilator-free days at day 28 (all secondary outcomes)
3. Dexmedetomidine was though associated with significantly more events of bradycardia, hypotension (no further info on the use of vasopressors) and asystoles (14 vs 2; 7 required mechanical resuscitation measures)

- DEX is an attractive sedative in certain situations (alcohol withdrawal, other forms of delirium, weaning process etc.), BUT
- DEX doesn't seem to provide any advantage in the sedation of mechanically ventilated patients in the ICU and
- Might be problematic due to adverse cardiovascular effects, especially in this group of patients
Shehabe et al. N Engl J Med 2019; 380:2506-2517
Did you Know?
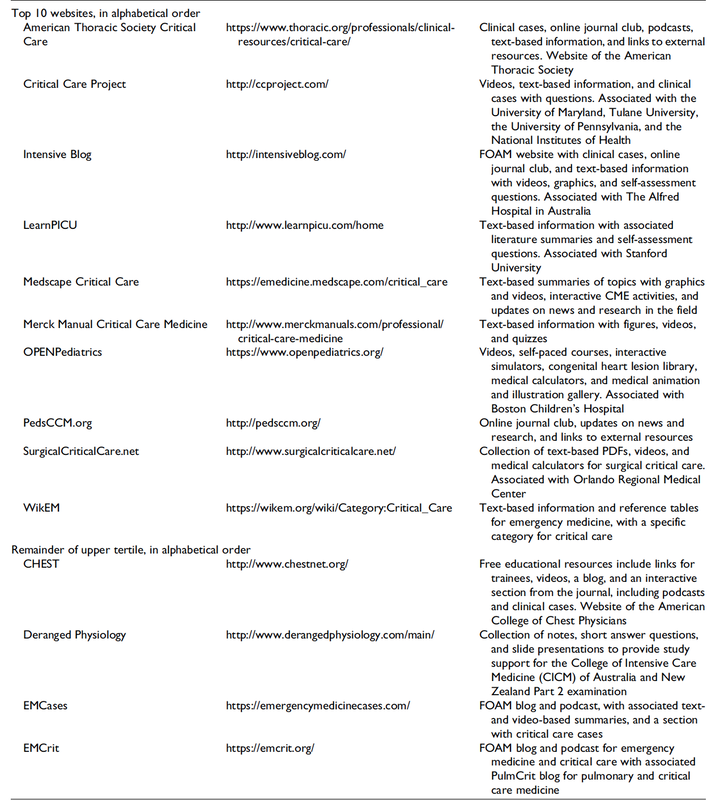
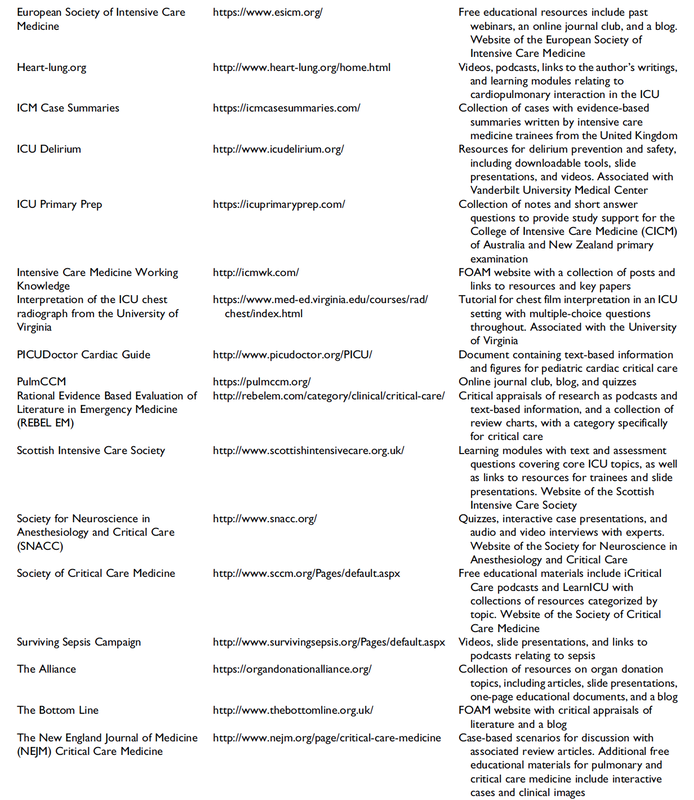
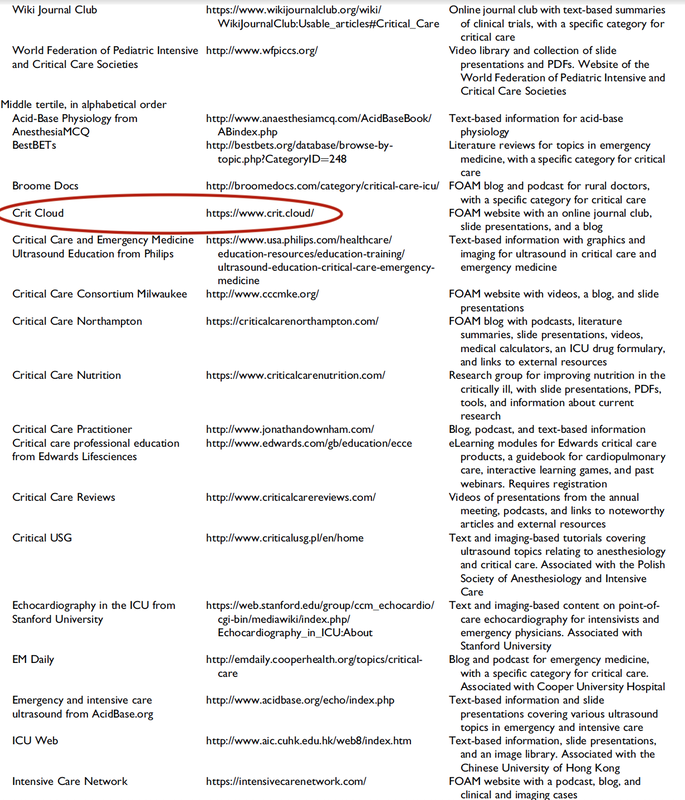
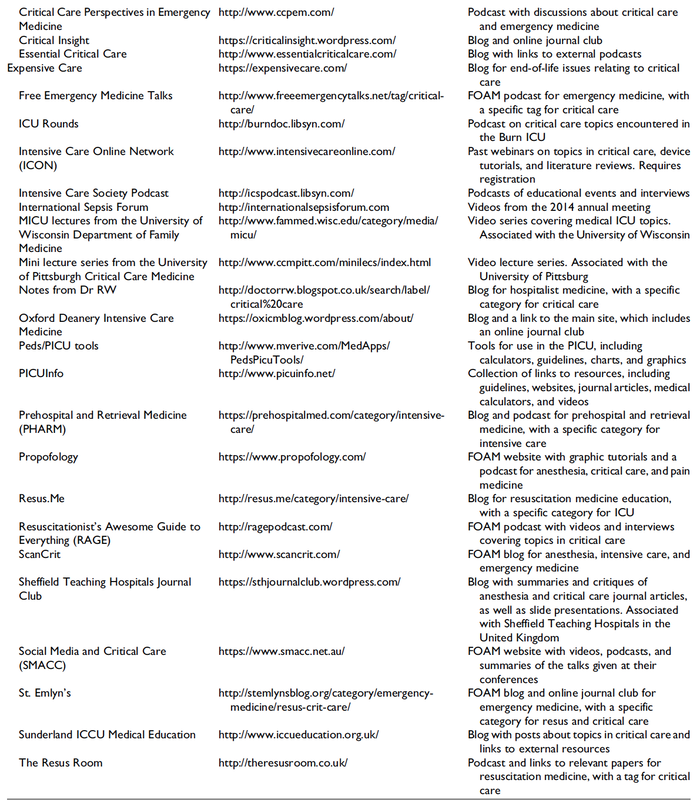
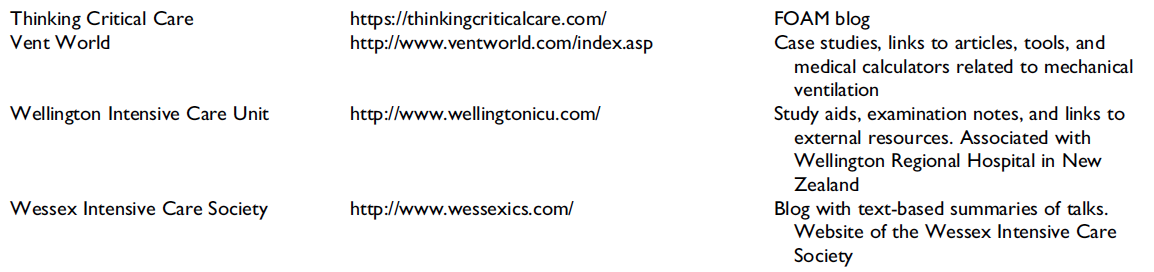
Top Ten Websites in Critical Care Medicine Education
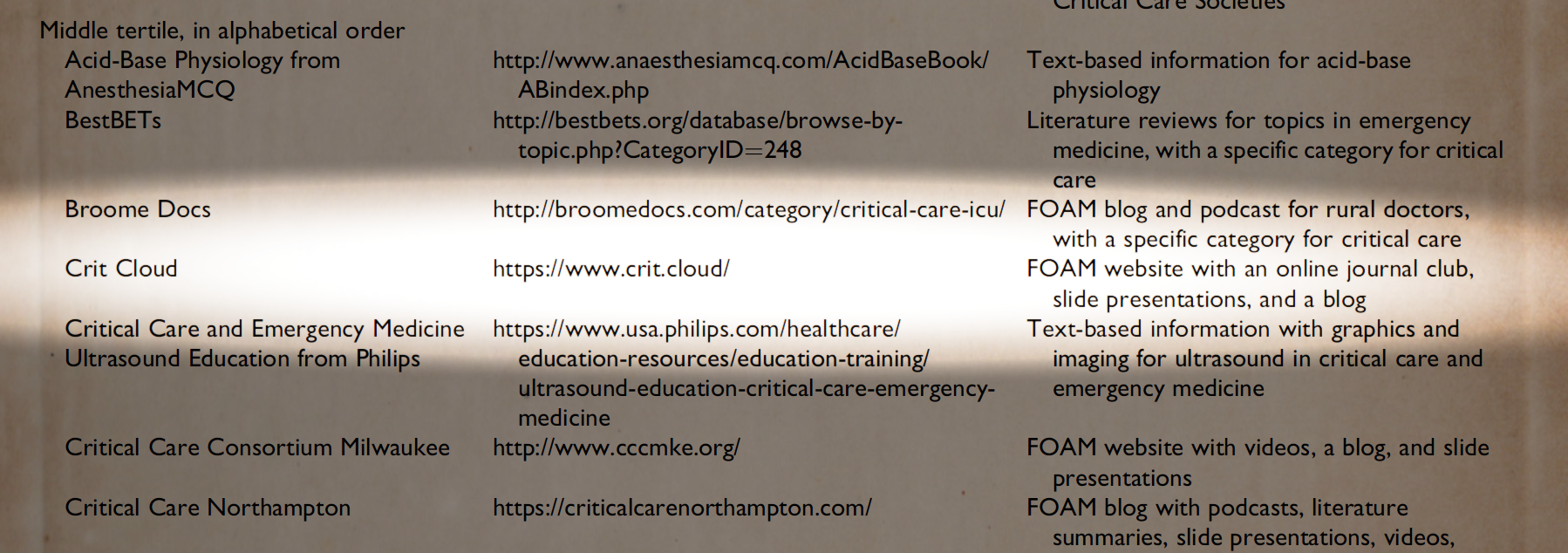
The Journal of Intensive Care Medicine has recently published a review of websites providing educational content that is part of the Free Open Access Meducation (FOAMed) movement. The authors have searched the web for critical care medicine education websites and have identified 97 sites they consider relevant for critical care.
These websites were then reviewed and evaluated using the Critical Care Medical Education Website Quality Evaluation Tool (CCMEWQET). They were then split up into three tertiles according to their score.
Congratulations to the Top Ten websites that indeed provide excellent educational information freely accessible.
Oh, and by the way we might mention that our small site Crit.Cloud has been considered among 96 other as relavant in this field and has ended up in the middle tertile with its ranking. 🙃
A big thank you to the authors of this paper for their excellent work and for providing us with an updated list of websites worth taking a closer look! We are delighted to follow their wish by sharing the table of these websites.
Wolbrink TA et al. J Intensive Care Med. 2018 Jan;34(1):3-16
Full List of all Website Reviewed (Click on a table enlarge)

Interestingly a discussion started on whether giving Lasix as a first line agent in the acute setting of pulmonary oedema is beneficial or not. A quick look into to current literature gave no clear answer and reading further into the topic revealed unusual properties of Lasix we hadn't been really aware of so far. We all use and love Lasix, but do we really know the drug?
The Beginning of Lasix
Furosemide (sometimes also called frusemide) was first developed by 'Farbwerke Hoechst AG' in Frankfurt am Main, Germany, a company that was founded back in the year 1863. Karl Stürm, Walter Siedel and Rüdi Weyer set the basis with the invention of N-substituted-3-Carboxy-6-Halo-Sulfanilamide, and it's derivates, one of them being furosemide. The researchers soon noticed its saluretic (sodium Na, potassium K and chloride Cl) and diuretic effect in almost equivalent proportions. As these substances did not cause any acidosis nor alkalosis, they suggested their future use for the treatment of oedema and hypertension.


Researchers soon noticed that the diuretic effect of furosemide lasted for about 6 hours... 'LAsts for SIX hours'... and therefore gave it the name: LASIX!
What is Furosemide
Furosemide is an organic anion from the group of loop diuretics (as are bumetanide and torasemide) and is sold under the brand name of Lasix©. Its indications are for the treatment of oedema due to heart or liver disease as well as kidney disease. It is also used for the treatment of mild or moderate hypertension. Furosemide has become one of the cornerstones in the treatment of heart failure.
Furosemide can be applied by oral intake as a tablet or as an intravenous injection. Once in the bloodstream, it is predominantly bound to proteins (>90%).
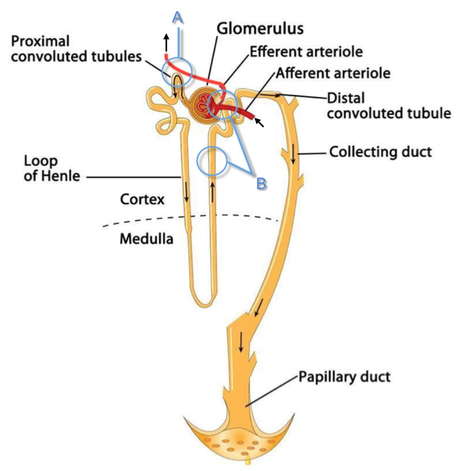
Loop diuretics do not undergo glomerular filtration. In fact, they pass the glomerulus and are actively secreted across proximal tubular cells by organic anion transporters and the multidrug resistance-associated protein 4 (area A). It is important to know that non-steroidal anti-inflammatory drugs (NSAID) and endogenous uremic anions compete with this loop diuretic secretion and can cause 'diuretic resistance'.
Once loop diuretics have reached the tubular system, they bind to sodium-potassium-chloride co-transporters (NKCC2) in the ascending limb of the loop of Henle and block the reabsorption of these ions directly (area B). Further down at the macula densa they inhibit the same co-transporter (area B) thereby stimulating renin secretion and inhibiting tubuloglomerular feedback. This results in preserved glomerular filtration despite increased salt delivery to the macula densa. All this finally results in the loss of sodium, chloride and potassium and therefore loss of water.
Furosemide also interacts with other sodium-potassium-chloride co-transporters (NKCC1) elsewhere in the body:
- Blocking NKCC1 in the ear probably explains the ototoxicity of loop diuretics
- Blocking NKCC1 in smooth muscle cells causes vasodilation
- Blocking NKCC1 in the afferent arteriole and near the macula densa elevates renin secretion and the generation of angiotensin II
These complex interactions on haemodynamics explain that the net response in each patient might be different. On the one hand, loop diuretics dilate blood vessels directly and increase the level of vasodilatory prostaglandins. On the other hand, some of these effects counteract each other making it difficult to predict which effect will finally predominate.
Many studies have looked closer into the vasoactive properties of furosemide. Current evidence indicates that it has a systemic venodilator effect which actually reduced preload acutely. The same investigators found a reduction in the right atrial pressure and the pulmonary capillary wedge pressure, presumably reflecting the systemic venodilator effect of furosemide.
While the acute venodilator effect may be beneficial to the failing heart, its action on arteries might be detrimental. Several studies have shown that in patients with chronic heart failure furosemide causes arterial vasoconstriction. Also, there is one study showing that pulmonary vascular resistance in healthy volunteers rose significantly.
Francis GS et al. described how the administration of furosemide actually led to decreased LV function, increased LV filling pressures, increases in MAP, SVR, plasma renin activity, and plasma noradrenaline levels.
Beneficial venodilator response predominates over arterial vasoconstriction in patients with (1) myocardial infarction and (2) salt depleted volunteers.
Venous relaxant effect has not been demonstrated in patients with chronic heart failure. In this setting detrimental arterial vasoconstriction seems to predominate.
Pardeep S et al. Br J Clin Pharmacol. 2000 Jul; 50(1): 9–13.
Francis GS et al. Ann Int Med 1985; 103(1): 1-6.
Pharmacological Properties
Administered furosemide orally has a limited and highly variable bioavailability. The diuretic effect starts within the first hour, and the duration of action is around 6 hours (4-8 hours). Injected furosemide intravenously is approximately twice as potent on a per-milligramme basis as oral doses.
In acute decompensated heart failure sodium retention becomes more avid and higher peak levels might be required to become more effective. This can be achieved by giving furosemide intravenously.
Once a loop diuretic is administered, the excretion of sodium chloride is increased for several hours. This is then followed by a period of very low sodium excretion resulting in a so-called 'post-diuretic retention'.
How to use Furosemide for Acute Decompensated Heart Failure (ADHF)
So far for the basics of furosemide, but what about its usage for acutely decompensated heart failure? Should furosemide be given as soon as possible or not?
The 2013 ACCF/AHA guidelines for the management of patients with heart failure give diuretics a class I recommendation. The evidence behind these recommendations though is level B or level C only! So these recommendations are not really helpful to answer this question.
The authors in UpToDate® mention diuretics directly after the use of oxygen. For patients with evidence of volume overload their recommendation is to give loop diuretics immediately (Grade 1B) as there is evidence that in this setting this may improve outcomes. They also suggest that patients with ADHF usually are volume overloaded, therefore indicating that most patients should receive diuretics ASAP.
The only exception they mention where some delay in inducing diuresis might be required is in patients with severe hypotension or cardiogenic shock.
There is reasonable doubt that patients with ADHF are usually volume overloaded, as suggested by UpToDate®. Zile MR et al. demonstrated that while most patients with acute pulmonary oedema have increased filling pressures, most did not have significant increases from their dry weight on presentation! Fallick et al. actually argue that it isn't fluid gain but rather shift in fluids from other compartments, mainly shift from the splanchnic circulation, which usually is very compliant.
And as mentioned above, there is evidence that giving a straight shot of furosemide might actually influence haemodynamics negatively in different ways (decreased LV function, increased LV filling pressures, increases in MAP, SVR, plasma renin activity and plasma noradrenaline levels).
In conclusion there is no straight forward answer to this question, but I would put it down as follows:

- Furosemide should not be routinely used for the immediate treatment of acute decompensated heart failure (ADHF)/ acute pulmonary oedema
- However, in patients with evidence of volume overload the administration of early furosemide (preferentially given as an intravenous bolus) seems beneficial and improves outcome. But beware, most patients are not volume overloaded!
- In urgent situations the focus should be on early non-invasive ventilation and the administration of nitroglycerin!
Wilson S et al., UpToDate.com 2018
WRITING COMMITTEE MEMBERS, Yancy CW, Jessup M, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation 2013; 128:e240.
Zile MR, Bennett TD, St John Sutton M, et al. Circulation 2008 Sep 30;118(14):1433-41
Fallick C et al. Circ Heart Fail 2011; 4: 669-75.

Thumbs up for Ket
Ketamine has kept its fascination in various settings, from retrieval medicine onto the the care of critically ill patients in the ICU. Ketamine reduces postoperative markers of inflammation, is a rapid-acting antidepressant drug with an effect lasting for several days and might have neuroprotective properties.
Ketamine also has become increasingly popular as an adjunct to other sedatives in the ICU. There is evidence showing that ketamine used in the ICU has the potential to reduce cumulative opioid consumption after surgery (Asad E. et al. J Intensive Care Med December 8 2015 ).
Even better: It does not cause any kidney injuries, preserves laryngeal protective reflexes, lower airway resistance and much more...
And: Ketamine is cheap and has been used safely for over 50 years by anaesthetists!
The Dark Side of Ket
But there's the other side of ketamine making all of this a little more complicated. After all, Ketamine is a psychoactive drug and has well known hallucinogenic properties. Developed in the 1960s as a dissociative anaesthetic agent it started to appear on the street in the early 1970s and made its way to the 1980s as Special K, Acid and Super C (Dotson JW et al. J of Drug Abuse, Vol 25, Issue 4, 1995).
From a medical point of view there are some worries that these psychotomimetic effects, which are of concern in the critically ill patient, might predispose to delirium (Erstad BL, J Crit Care, Oct 2016, Vol 35, p 145-149).
The PODCAST Trial
On the background of all this facts this trial revealed some interesting findings. Avidan et al. performed a
in which they randomly assigned
672 patients undergoing major cardiac and non-cardiac surgery under general anaethesia
into three groups to either receive a bolus of
placebo (normal saline), low-dose ketamine (0·5 mg/kg), or high dose ketamine (1·0 mg/kg) after induction of anaesthesia, before surgical incision.
Participants, clinicians, and investigators were blinded to group assignment. They found
NO difference in in the incidence of postoperative delirium among these groups
but
significantly more postoperative hallucinations and nightmares with increasing ketamine doses compared to placebo
Furthermore, postoperative pain was not influenced by giving a single dose of ketamine and this is in contrast to previous findings and current guidelines. Importantly, most of the previous studies are smaller than this trial, making these findings remarkable.
But what really drew my attention was the fact that the appearance of hallucinations and night-mares was increased for at least 3 days after surgery.
So if ketamine has no influence on postoperative delirium or pain but does induce hallucinations and nightmares, even 3 days after surgery, current guidelines might have to be revised.
The Bottom Line
- The application of a subanaesthetic dose of ketamine during surgery to tackle postoperative pain and delirium does not seem to be as effective as previously assumed
- The usage of ketamine in this setting even seems to have undesirable side-effects like hallucinations and nightmare - and this effect might even last for up to 3 days!
- This trial provides good reasons to look for other options to prevent postoperative delirium!
(Like dexmedetomidine? The answer to this question has just been answered: READ HERE!)
Well, it's not very often you read the term sepsis in the news but the word 'cure' causes estonishment or rather misbelief. Further reading certainly catches your attention: 'A doctor in the US state of Virginia claims to have found his own cure for sepsis' and 'Since then, he has used it to treat 150 sepsis patients. Just one has died of the condition, claims Dr Marik'. And it's not an article from some remote pseude magazine... no, it has been published in 'Chest'! And all this is not due to some novel molecule... it's all about Vitamin C!
Thanks to #FOAMed quite some smart brains have looked into this topic already...
So here's the most important facts you need to know - in short:
What's the Story?
single-centre retrospective cohort study
in which they have treated
47 consecutive septic patients over a periode of 7 months with intravenous vitamin C (1.5g 6-hourly), hydrocortisone (50mg 6-hourly) and thiamine (200mg 12-hourly)
and then compared these patients to
47 septic patients treated in their unit during the preceding 7 months
They performed
Propensity score matching
and found
An overall hospital mortality of 40.4% in the control group compared to 8.5% in the intervention group
This means
An absolute risk reduction of 31.9% and also according to the authors none of the patients in the intervention arm died of sepsis!
What Does This Mean?
There are several limitations that go hand in hand with studies as such and unblinded before-and-after studies have a lot. A major challenge in conducting observational studies is to draw inferences that are acceptably free from influences by overt biases, as well as to assess the influence of potential hidden biases. One of the biggest drawbacks in this current study is the timely/ seasonal difference when patients have been selected.
If you are interested to have a closer look on this you should read Dan's blog entry on stemlynsblog.org HERE.
Studies like this one are an important part of science, but observational studies are observational... not proof!
Why Vitamin C in Sepsis?
There are two rather small randomised control trials suggesting that vitamin C is safe in septic patients and might actually be of some degree of benefit for the patient.
Vitamin C
- Neutralizes free radicals and has therefore antioxydative properties
- Is an important conenzyme for the procollagen-proline dioxygenase, which itself is necessary for the biosynthesis of stable collagen in our body. Vitamin C deficiency leeds to unstable collagen and therefore scurvy
- Is an important cofactor in the synthesis of steroids like cortisol and catecholamines like dopamine and noradrenalin as well
- and it has many more functions that go beyond the scope of this blog entry!
However, the importance of vitamin C in the treatment and prevention of diseases like e.g. the common cold or influenza remains highly contrversial. The observation of some moderate positive influence on the course of disease in some studies could not be reproduced in other trials.
Under normal circumstances vitamin C deficiency is practically non-existent in Europe, but becomes a fact during sepsis. If this is clinically relevant in septic patients seems plausible but remains to be elucidated.
Shailja Chambial, Shailendra Dwivedi, Kamla Kant Shukla, Placheril J. John, and Praveen Sharma. Vitamin C in Disease Prevention and Cure: An Overview. Indian Journal of Clinical Biochemistry. Oktober 2013; 28(4): S. 314–328
H. Hemilä, E. Chalker: Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews. 2013
R. M. Douglas, E. B. Chalker, B. Treacy: Vitamin C for preventing and treating the common cold. In: Cochrane Database of Systematic Reviews. 2000; 2:CD000980.
Another great read into the details: Josh Farkas from pulmcrit
More Ifs and Buts
Paul Marik’s publication is interesting and deserves respect. It’s an observational study but provides no evidence by far. Vitamin C might be an interesting novel approach to sepsis but the term ‘cure’ used in the media is inappropriate and misleading.
The term ‘cure for sepsis’ also implicates that vitamin C is a cure for all infections causing sepsis and is therefore problematic.
The Current Bottom Line
- The study published by Marik et al. is purely observational and provides no proof at all.
- Just because vitamine C might be safe in Sepsis does not mean this has to be given. At this stage no recommendation can be made for the use of vitamin C in sepsis.
- Studies like these are an part of research itself - However, the use of the term 'cure' seem problematic and inappropriate in this context.
Marik et. al, J Chest 2017
The major problem is that performing a randomized controlled trial to elucidate the true incidence of contrast-induced nephropathy is considered unethical because of the presumption that contrast media administration is a direct cause of acute kidney injury.
While the discussion goes on Hinson et al. have come up with another nice piece of evidence that in emergency situations there is no reason to withhold the application of IV contrast for CT scans when required.
In this single-center retrospective cohort study researchers have included a total of 17'934 patient visits to their emergency department over a period of 5 years. They analysed three patient groups that where demographically similar: contrast-enhanced CT, unenhanced CT and no CT scan performed. Patients were included when their initial serum creatinine level was between 35 umol/L and 352 umol/L. Of all CT scans, 57.2 percent were contrast-enhanced. The probability of developing acute kidney injury was 6.8 percent for patients undergoing contrast-enhanced CT, 8.9 percent for patients receiving unenhanced CT and 8.1 percent for patients not receiving CT at all. This proofs to be the largest controlled study of its kind in the emergency department and shows that:
In current clinical context, contrast media administration for CT scans is NOT associated with an increased incidence of acute kidney injury. And even though a large randomised controlled trial is still missing it seems safe...
To Conclude:
There is no reason to withhold the use of IV contrast media in cases where contrast-enhanced CT is indicated to avoid delayed or missed diagnosis of critical disease.
Hinson J et al. Annals of Emergency Medicine, 2017; DOI: 10.1016/j.annemergmed.2016.11.021 OPEN ACCESS
Crit Cloud Review from 18/01/2015

While adrenaline is given for maximum vasoconstriction in order to promote coronary perfusion pressure CPP, amiodarone and sometimes lidocaine are used to promote successful defibrillation of shock-refractory ventricular fibrillation VF or pulseless ventricular tachycardia VT. While the usage of these drugs is undoubtedly very effective in patients with existing circulation the effectiveness during resuscitation remains a matter of debate.
The Effect of Adrenaline
As a matter of fact it has never been proven that adrenalin actually improves long-term outcome. In 2014 Steve Lin and colleagues published a systemativ review on the efficacy of adrenaline in adult out-of-hospital cardiac arrest (OHCA). They were able to show that according to current evidence standard dose adrenaline (1mg) improved rates of survival to hospital admission and return of spontaneous circulation (ROSC) but had no benefit in means of survival to discharge or neurologic outcomes.
What about Amiodarone and Lidocaine?
Kudenchuck et al. now made the effort to look into the efficacy of amiodarone and lidocaine in the setting of OHCA. Used according to the ACLS guidelines 2016 amidarone is given after the third shock applied when treating a shockable rhythm. Two rather small controlled trials have shown so far that using amidarone actually does increase the likelihood of ROSC and the chance to arrive at a hospital alive. It's impact on survival to hospital discharge and neurologic outcome though remains uncertain.
In this randomized, double-blind trial, the investigators compared parenteral amiodarone, lidocaine and saline placebo in adult, non-traumatic, OHCA. They ended up with 3026 patients meeting inclusion criteria and which were randomly assigned to receive amiodarone, lidocaine or saline placebo for treatment. They finally found that neither amiodarone nor lidocaine improved rate of survival to discharge or neurologic outcome significantly. There were also no differences in these outcomes between amiodarone and lidocaine. Across these trial groups also in-hospital care like frequency of coronary catheterisation, therapeutic hypothermia and withdrawal of life-sustaining treatments did not really differ, making a bias due to treatments after admission unlikely.
Take Home
- Amiodarone seems to improve the likelihood of ROSC and survival to hospital admission (similar to adrenaline)
- As there are no other options, I believe amiodarone should remain part of the standard treatment for shockable rhythms in OHCA
- Lidocaine can be safely removed from CPR sets as there is no benefit of over amiodarone
Read here:
N Engl J Med 2016;374:1711-22
Resuscitation, June 2014, Vol 85, Issue 6, p 732-740
New ACLS Guidelines 2015, The Changes

The Goodies of Ket
- Has no adverse effects on the gastrointestinal tract (bleeding) and does not cause acute kidney injury (compared to nonsteroidal anti-inflammatory drungs, NSAID's)
- Does not negatively influence bowel motility (in contrast to opioids)
- Preserves laryngeal protective reflexes
- Lowers airway resistance
- Increases lung compliance
- Is less likely to cause respiratory depression
- Is sympathomimetic, facilitates adrenergic transmission and inhibits synaptic catecholamine reuptake, therefore increasing heart rate and blood pressure
The Concerns of Ket
- Might increase pulmonary airway pressure and therefore aggravate pulmonary hypertension
- Might cause well known psychotomimetic effects which are of concern in the critically ill patient as this might predispose to delirium
- Interacts with benzodiazepines via the P450 pathway which could result in drug accumulation and prolonged recovery
Concerns Proven Wrong
- Current evidence shows no increased intracranial pressure or associated adverse neurologic outcomes associated with ketamine administration in critically ill patients
Take Home
Taking precautions and contraindications into account ketamine is considerably safe and even avoids potentially adverse side effects of other agents used.
Erstad BL, J Crit Care, Oct 2016, Vol 35, p 145-149
Search
Translate
Select your language above. Beware: Google Translate is often imprecise and might result in incorrect phrases!

Categories
All
Airway
Cardiovascular
Controversies
Endocrinology
Fluids
For A Smile ; )
Guidelines
Infections
Meducation
Neurology
Nutrition
Pharmacology
Procedures
Radiology
Renal
Respiratory
Resuscitation
SARS CoV 2
SARS-CoV-2
Sedation
Sepsis
Transfusion
Archives
January 2021
September 2020
March 2020
February 2020
January 2020
December 2019
November 2019
July 2019
May 2019
March 2019
February 2019
January 2019
December 2018
January 2018
October 2017
August 2017
June 2017
March 2017
February 2017
January 2017
October 2016
July 2016
June 2016
April 2016
February 2016
December 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
Author
Timothy Aebi
 RSS Feed
RSS Feed


