 When the FDA approved dexmedetomidine (DEX) in 1999, intensive care medicine had a novel and highly promising drug at its disposal. Compared to clonidine, dexmedetomidine is an 8 times more selective, central alpha 2 agonist, which binds to all 3 subtypes of the receptor. The properties of this substance were auspicious, among them: sedation, analgesia, neuroprotective effects and a lack of respiratory depression. - Sedation decreases sympathetic activity, aggression and leads to a non-REM-like state, which of all sedatives comes closest to natural sleep. Cognitive functions are maintained, and patients usually remain arousable. - Dexmedetomidine has a particular analgesic effect via modulation in the region of the posterior horn of the spinal cord. This has shown to reduce the use of opiates. - By reducing cerebral catecholamines, dexmedetomidine exerts a neuroprotective effect. - Interestingly, sedation with dexmedetomidine is not associated with significant respiratory depression. These properties pointed to a wide range of applications in the intensive care unit: - Sedation in patients with non-invasive ventilation - Weaning of invasively ventilated patients - Agitated delirium - Treatment of various withdrawal syndromes - Fiberoptic awake intubation in theatre conditions Dexmedetomidine comes with its side effects, though. Most commonly bradycardia and hypotension are observed, making second and third-degree heart block a contraindication. Also, nausea and a dry mouth might be seen. Interestingly, prolonged use might be associated with some extent of discontinuation syndrome similar to clonidine. This involves hypertension, tachycardia, nervousness etc. What Evidence Do We Have So Far? |
The SPICE III Trial |  |
Precisely this question was now addressed by Shehabi et al., published in the NEJM
They performed an
International (8 countries, 74 ICU's), randomised controlled, unblinded trial
In which they evaluated
4000 ICU patients that were expected to need mechanical ventilation for at least 48 hours and required sedation for safety or comfort
They compared
Patients sedated with propofol, midazolam or other agents as prescribed by the treating physician with patients receiving dexmedetomidine as a continuous infusion
(if DEX alone was insufficient, other agents could be added! In fact, 64% of patients also received propofol, 3% midazolam and 7% received both)
They found
1. No difference in 90-day mortality (primary outcome) and
2. No difference in death after 180 days, institutional dependency at 180 days, mean cognitive decline and assessment of the quality of life. Also no difference in median days free from coma to day 28 and median ventilator-free days at day 28 (all secondary outcomes)
3. Dexmedetomidine was though associated with significantly more events of bradycardia, hypotension (no further info on the use of vasopressors) and asystoles (14 vs 2; 7 required mechanical resuscitation measures)

- DEX is an attractive sedative in certain situations (alcohol withdrawal, other forms of delirium, weaning process etc.), BUT
- DEX doesn't seem to provide any advantage in the sedation of mechanically ventilated patients in the ICU and
- Might be problematic due to adverse cardiovascular effects, especially in this group of patients
Shehabe et al. N Engl J Med 2019; 380:2506-2517
Did you Know?

On arrival to our ICU, the patient was noted to be still unresponsive. He showed no reaction to painful stimulation. The Pupils were rather wide, but symmetrical in size and showed a prompt response to light. Brain stem reflexes were present and peripheral reflexes were triggerable. His breathing pattern was regular, and saturation levels were above 96% on room air. A blood gas analysis showed a normal pH and normal CO2-levels.
As usual, the common reflexes started to kick in, and some suggested to go for a CT-scan of his head to out-rule some significant complications. Luckily enough, close observation revealed some slow improvement of his alertness, and we considered the possible diagnosis of a central anticholinergic syndrome (CAS).
After the application of 1mg of physostigmine (2x0.5mg) intravenously the patient almost promptly awoke and had an uneventful stay on our unit.
This case just reminded me of these many patients in anaesthesia that inexplicably show delayed awakening after sedation or a general anaesthetic.
In fact, it is estimated that the incidence of central anticholinergic syndrome is around 8- 12 % following general anaesthetic and lesser with regional anaesthesia.
What is a Central Anticholinergic Syndrome?

Classically the central anticholinergic syndrome (CAS) describes a condition where a substance causes a competitive antagonism of acetylcholine (ACh) at peripheral and central muscarinic receptors. Initially, these were plants containing atropine, hyoscyamine and scopolamine.
There are four muscarinic receptors:
- M1 mainly in the central nervous system (responsible for delirium when antagonised)
- M2 in the brain and heart
- M3 in the salivary glands and
- M4 in the brain and lungs
The PERIPHERAL SYNDROME presents with:
- Dry mouth
- Difficulty swallowing (lack of saliva)
- Photophobia and blurred vision (due to dilated pupils)
- Dry skin, fever
- Reduced bowel sounds and urinary retention
The CENTRAL SYNDROME presents with:
- Agitation, agitated delirium, visual and auditory hallucinations
- Hypoactive delirium may also occur, this seems to be more common though in the postoperative setting
The clinical diagnosis of a CAS is more straightforward when typical peripheral symptoms accompany central signs.
The Problem with the "Silent" Postoperative CAS
The clinical diagnosis of a CAS is often straight forward when typical central symptoms accompany peripheral symptoms. The problems are patients in the postoperative setting, in which the patient often presents with somewhat atypical central symptoms and often minimal or even no peripheral symptoms at all.
Especially in this setting, the anticholinergic syndrome may be accompanied by sedation or coma. The mechanisms causative for this phenomenon are not well understood but might include greater tolerance at peripheral receptors, longer persistence at central receptors or greater CNS susceptibility due to age or disease.
Postoperative CAS is often associated with atypical central symptoms and minimal or even no peripheral signs at all! Sedation and coma are often observed in this setting.
What Drugs Cause CAS?
Common anticholinergics agents should be more accurately referred to as antimuscarinics, as these agents do not generally block nicotinic receptors.
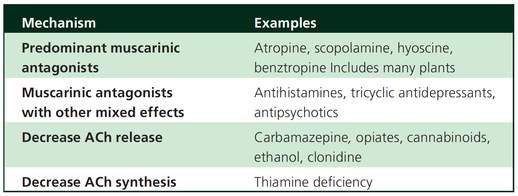
The Problem is that many currently used drugs in anaesthesia and critical care are also known to cause this syndrome.
This includes:
Benzodiazepines, opioids, phenothiazines, butyrophenones, ketamine, etomidate, propofol, nitrous oxide, and volatile inhaled anaesthetics!
How Can I Diagnose a "Silent" Postoperative CAS?
The fact that postoperative CAS often lacks the presence of peripheral symptoms makes the diagnosis challenging. The different presentation of the syndrome ranging from somnolence, confusion, amnesia, delayed recovery, stupor, coma to agitation, hallucinations, dysarthria, ataxia, delirium makes it difficult to diagnose accurately.
It is, therefore, a diagnosis of exclusion! The most helpful tool you have is physostigmine!

The prompt arousal of a patient after the application of intravenous physostigmine is highly suggestive of a postoperative central anticholinergic syndrome.
How to Use Physostigmine
When dealing with prolonged somnolence or unexplained agitation following any form of anaesthesia, make sure to check and monitor vital signs and provide basic or advanced life support if necessary.
Exclude common causes first (e.g. overhang of sedatives or opioids, persistent muscular paralysis, hypoxemia, hypercapnia, hypoglycemia and other).
If common causes can be excluded and CAS is a probable diagnosis, you should consider the application of intravenous physostigmine.
Physostigmine in recommended doses is considered safe! Possible adverse effects are considered unlikely. Studies found cholinergic symptoms sometimes to be mild, and these adverse effects are more an indication of probable excessive doses rather than an established safety concern.
For postoperative CAS a dose of 1mg of physostigmine i/v is recommended.
This dose can be divided into two doses of 0.5mg i/v if required.
The maximum dose recommended in this setting is 2mg i/v.

Beware: You are giving Physostigmine Salicylat - Do not give to patients with aspirin allergy!

The Goodies of Ket
- Has no adverse effects on the gastrointestinal tract (bleeding) and does not cause acute kidney injury (compared to nonsteroidal anti-inflammatory drungs, NSAID's)
- Does not negatively influence bowel motility (in contrast to opioids)
- Preserves laryngeal protective reflexes
- Lowers airway resistance
- Increases lung compliance
- Is less likely to cause respiratory depression
- Is sympathomimetic, facilitates adrenergic transmission and inhibits synaptic catecholamine reuptake, therefore increasing heart rate and blood pressure
The Concerns of Ket
- Might increase pulmonary airway pressure and therefore aggravate pulmonary hypertension
- Might cause well known psychotomimetic effects which are of concern in the critically ill patient as this might predispose to delirium
- Interacts with benzodiazepines via the P450 pathway which could result in drug accumulation and prolonged recovery
Concerns Proven Wrong
- Current evidence shows no increased intracranial pressure or associated adverse neurologic outcomes associated with ketamine administration in critically ill patients
Take Home
Taking precautions and contraindications into account ketamine is considerably safe and even avoids potentially adverse side effects of other agents used.
Erstad BL, J Crit Care, Oct 2016, Vol 35, p 145-149

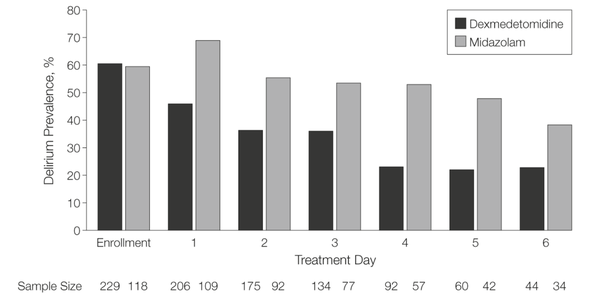
I've stepped over this prospective, double-blind, randomised trial by Riker et al. in which 68 centres in 5 countries recruited intubated 366 patients to received moderate to light sedation with either dexmedetomidine or midazolam. All patients received daily arousal assessment.
Their primary end point was the percentage of time within the target sedation range (RASS score −2 to +1) and this did not differ between the two groups.
Looking at the secondary endpoints though make things a lot more interesting. Just before the beginning of the sedation period both groups had a similar prevalence of delirium. During study drug administration though, the effect of dexmedetomidine treatment on delirium was significant. A reduction of 24.9% with dexmedetomidine is rather impressive (see figure below). This effect was even greater in patients who were CAM-ICU-positive at baseline.
Finally patients on dexmedetomidine had shorter time to extubation (1.9 days in average) while their length of stay on ICU did not differ.
From a safety point of view the most common adverse effect of dexmedetomidine was bradycardia. It's noteworthy that patients on midazolam had more episodes of hypotension and tachycardia.
THE BOTTOM LINE
- This is another study indicating that dexmedetomidine seems to be beneficial in regards of delirium in mechanically ventilated patients and might speed up time to extubation
- Dexmedetomidine is safe in patients where moderate to light sedation is the aim
Riker et al. JAMA. 2009;301(5):489-499. doi:10.1001/jama.2009.56 OPEN ACCESS
Read more HERE on BIJC

+++ Anaesthesiologists are opening private clinics for off-label infusions of ketamine for depression http://bit.ly/1IGYTcI +++ Dr. Jim Roberts says #ketamine is an ideal treatment for excited #delirium: http://emn.online/Dec15InFocus +++ Major #ketamine treatment trial to start in 2016 http://m.huffpost.com/au/entry/8501942 +++ More impressed every day with low dose ketamine for pain management! https://www.youtube.com/watch?v=DgckjVVBb48 ...
Intravenous ketamine is also used in critical care units and to my knowledge most clinicians use ketamine as an adjunct to other sedatives. This might be for patients on mechanical ventilation, intubation procedures or simply as an additive to a patient-controlled analgesia pump. I personally think ketamine is one of the essentials in ICU's, but what does the evidence say.
Asad et al. have performed a systematic review on the usage of ketamine as a continuous infusion (>24h) in intensive care patients. The aim was to find evidence in favour for the utilisation of ketamine in the ICU.
As a result of this review - current evidence suggests that:
- In critically ill postoperative patients ketamine has the potential to reduce the cumulative morphine consumption at 48h compared to morphine only
- Several trials show the potential safety of ketamine in regards of cerebral haemodynamics in patients with traumatic brain injury, improved gastrointestinal motility and decreased vasopressor requirements
- One observational study and case reports suggest that ketamine is safe, effective and may have a role in patients who are refractory to other therapies
Our conclusion: THUMBS UP for ketamine in the ICU
Asad E. et al. J Intensive Care Med December 8, 2015
To make it short: Ketamine does not increase ICP in comparison to opioids. They conclude that ketamine should not be discouraged on the basis of ICP-related concerns.
Wang et al. J Anaesth. 2014 May 24

While initially described in children and traumatic brain injury it is also increasingly reported in other critically ill patients. If you are interested in some background information on this syndrome this recent case report by Mayette et al., published in the Annals of Intensive Care, provides an interesting insight in this topic.
Parke et al. BMJ. 1992;305:613
Mayette M. et al. Ann Intensive Care. 2013 Sep 23;3(1):32
Take Home Message: Risk factors for PRIS appear to be...
- Children (under 16 yrs of age)
- Propofol dose in excess of 5 mg/kg/hr
- Continuous infusion > 48 hrs
- Co-administration of catecholamines and corticosteroids
Search
Translate
Select your language above. Beware: Google Translate is often imprecise and might result in incorrect phrases!

Categories
All
Airway
Cardiovascular
Controversies
Endocrinology
Fluids
For A Smile ; )
Guidelines
Infections
Meducation
Neurology
Nutrition
Pharmacology
Procedures
Radiology
Renal
Respiratory
Resuscitation
SARS CoV 2
SARS-CoV-2
Sedation
Sepsis
Transfusion
Archives
January 2021
September 2020
March 2020
February 2020
January 2020
December 2019
November 2019
July 2019
May 2019
March 2019
February 2019
January 2019
December 2018
January 2018
October 2017
August 2017
June 2017
March 2017
February 2017
January 2017
October 2016
July 2016
June 2016
April 2016
February 2016
December 2015
October 2015
September 2015
August 2015
July 2015
June 2015
May 2015
April 2015
March 2015
January 2015
December 2014
November 2014
October 2014
September 2014
August 2014
July 2014
June 2014
May 2014
April 2014
March 2014
February 2014
January 2014
December 2013
November 2013
Author
Timothy Aebi
 RSS Feed
RSS Feed


