 Anaemia is a very common finding in critically ill patients and the idea to Supplement IV iron in these patients sounds tempting. Intravenous iron preparations are licensed for patients with iron deficiency anaemia when oral iron preparations are ineffective or contraindicated. The question is whether IV iron is also helpful in the critically ill.
Pieracci et al. have looked at this question more precisely and published their results in Critical Care Medicine. In their multicentre, randomized, single-blind, placebo-controlled study they enrolled a total of 150 critically ill trauma patients in which baseline iron markers were consistent with functional iron deficiency anaemia. They randomized patients to either receive iron sucrose 100mg IV or placebo three times a weeks for up to 2 weeks. They found that treatment with IV iron increased ferritin concentration significantly but had no effect on transferrin saturation, iron-deficient erythropoiesis, haemoglobin concentration or packed RBC transfusion requirement. In conclusion: IV iron supplementation in anaemic, critically ill trauma patients cannot be recommended. Pieracci F et al. Crit Care Med, September 2014 - Volume 42 - Issue 9 - p 2048–2057  Thoracocentesis is a procedure often used to further determine pleural effusions. This commonly performed procedure may lead to complications including the development of a pneumothorax. Wilcox et al. performed a systematic review in JAMA of current literature to answer following two questions: 1. What are the most accurate diagnostic indicators to diagnose an exsudate? and 2. What are the most common adverse side effects and factors affecting them?
48 studies were included to answer the first question, while 37 studies were used to approach question number 2. In conclusion: - Light's criteria, pleural fluid cholesterol (<55 mg/dl) and pleural fluid LDH (>200 U/L) levels, and the pleural fluid cholesterol to serum cholesterol ratio (> 0.3) are the best diagnostic indicators for pleural exsudates - Pneumothorax was the most common complication of thoracocetesis (incidence 6%). Chest tube placement was needed in 2% of all procedures. And most impressive: Ultrasound skin marking by a radiologist or ultrasound-guided thoracocentesis were not associated with a decrease in pneumothorax events. ... would you abandon the ultrasound? Wilcox et al. JAMA, June 18, 2014, Vol 311, No. 23  In the most recent edition of 'Continuing Education in Anaesthesia, Critical Care and Pain' there is a very good overview article on rapid sequence induction (RSI) and its place in modern anaesthesia. Wallace and McGuire also critically look at cricoid pressure (CP) as a part of classical RSI. In their publication they state that "there have been no prospective randomized clinical studies performed to prove the clinical hypothesis and the level of evidence to support the use of cricoid pressure is poor (Level 5)". Level 5 corresponds to 'Expert Opinion' (see table below). They also mention that aspiration has occured despite CP, that CP is often poorly performed, that it may hinder bag-valve mask ventilation as well as LMA insertion and that is may worsen laryngoscopy. It's mentioned that "Critically, it has also been shown to potentially obstruct the upper airway and reduce time to desaturation". 'This is nothing new' you might say. Why am I mentioning this? Well, the remarkable thing about this article is the fact that it was published in a Journal that is a joint venture of the British Journal of Anaesthesia BJA and The Royal College of Anaesthetists in collaboration with the Intensive Care Society and Pain Society. Considering the fact that The NAP4 guidelines continue to support its use as part of an RSI and as such, it is still considered a standard of care in the UK and therefore also Ireland, this publication might indicate some change in mind... or not? The authors summarize: Application of cricoid pressure is advisable — unless it obscures the view at laryngoscopy or interferes with manual ventilation or supraglottic airway device placement. I personally still would want to know what exactly makes a 'Level 5' medical intervention 'advisable' especially in regards of all the possible problems and complications associated with it. Wallace et al., Continuing Education in Anaesthesia, Critical Care & Pain, Volume 14(3), June 2014, p 130–135 Read our previous BIJC post: Cricoid Pressure for RSI in the ICU: Time to Let Go? (Updated) 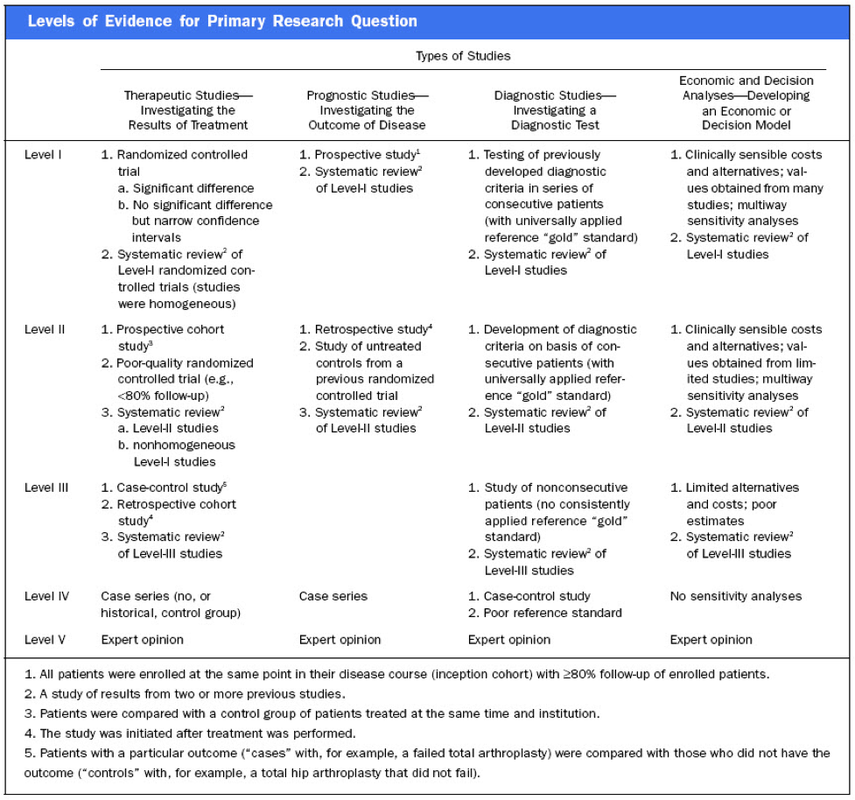 Simply Great and Helpful: Normogram for Calculating the Maximum Dose of Local Anaesthetics20/5/2014
 While many medical articles conclude 'more research is needed...', or further study is required' here comes a straight forward article that gives you a simple, but very helpful tool for your daily work. In this month's Anaesthesia Williams and Walker present a normogram for calculation of the maximum safe volume (ml) of local anaesthetic to a clinical acceptable degree of accuracy. Indeed this normogram allows you to find out the various doses within a few seconds. In their article they looked at 14 commonly used local anaesthetics and provide some further background information. The normogram only works with body weights up to 70kg, but they recommend to use the ideal body weight for obese patients. An article worth reading (open access!) and a normogram worth using! Williams DJ et al. Anaesthesia. doi: 10.1111/anae.12679 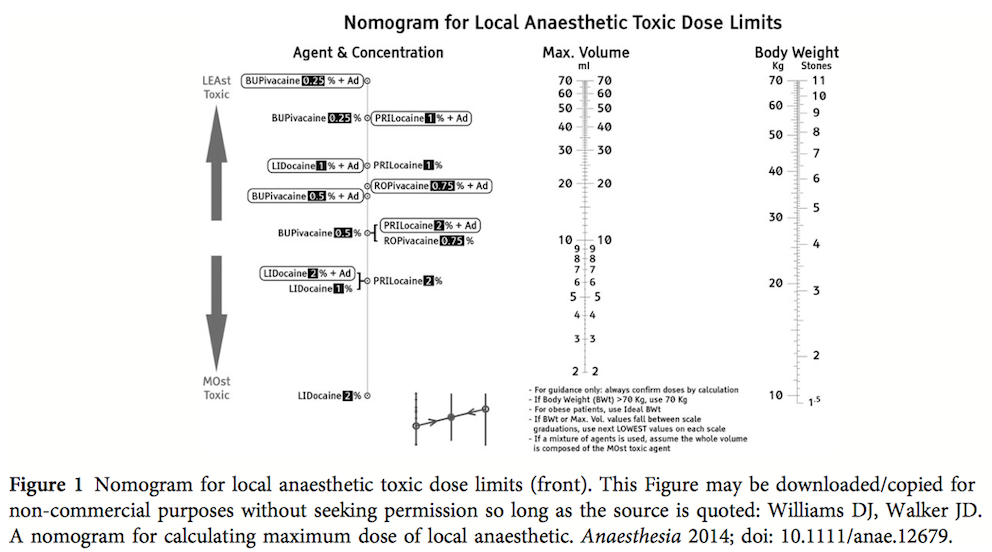 One of the Big Mysteries Solved: How to Correctly Prescribe the Duration of Antibiotic Treatments2/5/2014
 Just this week the World Health Organisation WHO has issued a warning that resistance of organisms to antibiotics will become one of the biggest challenges of the upcoming decade. Indeed, the correct prescription of antibiotics is crucial for successful treatment and the WHO states that completing the full length of the treatment is just as important.
But what is actually the correct length of treatment for all the different antibiotics and diseases? How many ward rounds on ICU's have I spent with microbiologists (the maybe most important specialists on our sides!) wondering on how they always had a straight answer on the correct length of treatment. 7 days, 10 days or sometimes 21 days... a little mystery to most intensivists, until now! Hitchhiking though the the wide space of the internet I finally found secret to this question. Back in the year 2010 Paul E. Sax, a Professor of Medicine at Harvard Medical School him self, posted an excellent blog for the NEJM Journal Watch website. Inspired by a New York Time article by Harvard Professor Daniel Gilbert he finally gave insight into one of the great mysteries of medicine: To figure out how long antibiotics need to be given, use the following rules:
That did not occur by chance Wow, not much more I can add! Paul E. Sax, NEJM Journal Watch HIV/AIDS Clinical Care, October 22nd 2010 NYT article by Daniel Gilbert from October 2010  Guidelines on advanced cardiopulmonary resuscitation around the world, including the ACLS guidelines, are based on four important concepts: mechanical resuscitation (CPR), defibrillation, airway management and also application of vasoactive drugs. The application of these drugs is intended to improve hemodynamics and the heart's responsiveness to defibrillation.
What some of us might not be aware of though, but has already been mentioned by the '2010 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations' and the 'European Resuscitation Council Guidelines' in 2010: There is actually no definitive evidence that the application of these drugs provides any long-term benefit for these patients. While vasopressors are intended to improve coronary and cerebral perfusion and therefore successful defibrillation and neurological outcome, there is actually some concern (animal and registry studies) that this might actually decrease microcirculation and cerebral blood flow as well as increase myocardial oxygen consumption and cause post-defibrillation ventricular arrhythmias. Also the use of anti-arrhythmic drugs as well as their combination with vasopressors lacks evidence of any impact on survival. Another interesting fact is that we have no idea about ideal dosage or optimal timing of these drugs... should they be given continuously? This and many more questions and facts are discussed in an interesting review article by Sunde and Olasveengen in Current Opinion in Critical Care. They conclude that there is no evidence to support any specific drugs during cardiac arrest and that healthcare systems should not prioritise implementation of unproven drugs before good quality of care can be documented. Are we heading towards an era of drug-free resuscitation? Sunde K et al. Curr Opin Crit Care. 2014 April 16 Article accessible here  Most of us being trained as anaesthetists in the last couple of years have learnt to perform a rapid sequence induction (RSI) including the application of cricoid pressure (aka the Sellick manoeuvre) in order to prevent aspiration of gastric content.
Over the last couple of years though this manoeuvre has been seriously questioned as scientific evidence is lacking and there are concerns that cricoid pressure might actually be potentially harmful. A lot has been written on this topic so far and some great reviews can be found easily on the internet thanks to the concept of Open Free Access Meducation (FOAMed, see below). Still I would like to add some thoughts on to this discussion and maybe mention one or two more interesting facts. Cricoid pressure was actually first described by Sellick in the Lancet in 1961 as a preliminary report and basically represented an un-controlled case study in which no or only insufficient information on the studies patient population was provided. There was no standardisation of the force for cricoid pressure as of the medications used for induction. There was also no information on the quality of laryngoscopy and intubation. Steinmann and Priebe (abstract in english) have exactly analysed this publication and found some relevant methodological shortcomings. It is therefore remarkable that this publication led to an anaesthetic dogma practised all over the world. As mentioned in the European Resuscitation Council Guidelines of 2005, studies in anaesthetised patients show that cricoid pressure impairs ventilation in many patients, increases peak inspiratory pressures and causes complete obstruction in up to 50% of patients depending on the amount of pressure applied (Petito, Lawes, Hartsilver, Allman, Hocking, Mac, Ho, Shorten). The incidence of a difficult intubation is significantly higher in preclinical emergency situations than in an elective theatre environment (Timmermann A et al. Resuscitation 2007;70(2):179-185). It is therefore possible, that cricoid pressure itself actually is one of the reasons why unexperienced emergency physicians experience additional difficulties when intubating 'in the field'. One concern often mentioned is the fear that non-adherence to current guidelines by not applying cricoid pressure might have adverse legal implications. But what do current guidelines actually say? Priebe et al. partially looked at this in 2012. Several guidelines indeed still recommend cricoid pressure, sometimes even with less force in the awake patient. But some guidelines have started to implement current evidence. The 2010 Clnical Practice Guidelines on General Anaesthesia for Emergency Situations by the Scandinavian Society of Anaesthesiology and Intensive Care Medicine state following: (i) The use of CP cannot be recommended on the basis of scientific evidence (recommendation E, supported by non-randomized, historic controls, case series, uncontrolled studies and expert opinion) (ii) The use of CP is therefore not considered mandatory but can be used on individual judgement (recommendation E). (iii) If facemask ventilation becomes necessary, CP can be recommended because it may reduce the risk of causing inflation of the stomach (recommendation D, supported by non-randomized, contemporaneous controls) The 2005 European Resuscitation Council Guidelines (page 1322, pdf here) puts it this way: - The routine use of cricoid pressure in cardiac arrest is not recommended. - Studies in anaesthetised patients show that cricoid pressure impairs ventilation in many patients, increases peak inspiratory pressures and causes complete obstruction in up to 50% of patients depending on the amount of cricoid pressure (in the range of recommended effective pressure) that is applied. Still though it has to be mentioned that the Difficult Airwas Society (DAS) continues to recommend cricoid pressure for RSI on it's website. The current recommendation though seems to date back to 2004 and the question is mentioned on their website whether any pressure should be applied before loss of consciousness. Also the Association of Anaesthetists in Great Britain and Ireland recommends cricoid pressure in their AAGBI Safety Guidelines of 2009 on pre-hospital anaesthesia. It is also mentioned that 'badly applied cricoid pressure is a cause of a poor view at laryngoscopy. It may need to be adjusted or released to facilitate intubation or ventilation'. While the discussion on this issue in adults will continue the dogma of cricoid pressure might soon fall in paediatric patients as Neuhaus D et al. published a Swiss trial in 2013 where they could show that a controlled rapid sequence induction without cricoid pressure is actually safe. Further research is on its way: Trethrewy E et al. Trials. 2012 Feb 16;13:17. Until then it seems as if we are faced with guidelines mostly still in favour for cricoid pressure and evidence based medicine, which is rather discouraging us of further performing this procedure. It is good practice to constantly question current guidelines and further improve them for the patient's sake. Indeed you have to ask yourself on how far you want to stick to current guidelines for legal reasons or if you change your practice according to emerging evidence. Some of the hospitals I worked at in Switzerland have stopped performing cricoid pressure for RSI some years ago and haven't encountered any worsening in their patient outcomes. Taking into account that most RSI in the ICU resemble emergency intubations out of hospital rather than the controlled environment of a theatre I feel there are good reasons to start re-evaluating and possibly change current guidelines. Other very interesting resources of information can be found here (FOAMed): - lifeinthefastlane.com on cricoid pressure - resus.me on cricoid pressure - Update 02/05/14: Minh Le Cong published a statement of the NAP 4 investigators on his blog website: statement from NAP 4 (on prehospitalmed.com) ... The discussion goes on!  Intensivists have repeatedly been warning on the potential effect side effects when infusing bigger quantities of normal saline like acidosis and potentially worse outcomes. It is well recognized that infusion of normal saline can lead to metabolic acidosis, but the link between the acidity of saline solution and the acidaemia it can produce might be not straightforward!
This article from the beginning of this year shows a surprising insight on the various components involved when using normal saline infusions and comes to the conclusion that the acidaemia complicating saline infusions is actually unrelated to the acidity of the normal saline solution itself. It turns out that in vitro the acidity of a normal saline solution is mainly due to dissolved CO2 and PVC degradation of the bag containing the solution. The metabolic acidosis by saline infusions in vivo though mainly results from from buffer base dilution and is not directly related to the pH of the infusion at all. Got interested? Reddi B, et al. Int J Med Sci. 2013 Apr;10(6):747-50  Inspired by an excellent post by Dr. Pat Nelligan on AnaesthesiaWest we would like to provide even more evidence against routine change of IV catheters... just because you are told to do so for hospital policy reasons.
Brown D. et al. have provided an excellent overview article on this issue. It is clearly shown that peripheral IV catheter should be replaced as clinically indicated, rather than on a routine basis. The level of evidence here is: A. This means that this recommendation of this treatment/ procedure is effective! We add another 3 articles supporting this recommendation. We do many other things on ICU with lower levels of evidence, or even no evidence at all. So it is definitely time to change this bad habit. So Pat, I won’t do it either... full stop! Bregenzer T, et al. Arch Intern Med, January 1998; 158(2):151-6 Lee WL, et al. Am J Infect Control, 2009 Oct;37(8):683-6 Lai KK, et al. Am J Infect Control, 1998 Feb;26(1):66-70 |
Search
|

 RSS Feed
RSS Feed


